

Angioplasty and stenting in carotid dissection with or without associated pseudoaneurysm
- PMID: 16219841
- PMCID: PMC7976134
Angioplasty and stenting in carotid dissection with or without associated pseudoaneurysm
Abstract
Background and purpose: Carotid angioplasty and stent placement may be the preferred treatment in patients with carotid dissection who have failed medical management. The goal of this study was to determine the procedural feasibility and safety as well as long-term complication rates of carotid angioplasty and stent placement in a consecutive cohort of relatively young, high-surgical-risk patients.
Patients and techniques: A series of 26 consecutive patients (mean age, 49 years; 15 men and 11 women) who underwent angioplasty and stent placement for carotid dissection with or without pseudoaneurysm from April 1997 to April 2005 at our institution (9 traumatic, 8 spontaneous, and 9 iatrogenic) was retrospectively reviewed. Twenty-eight stents were used in 29 procedures performed on 27 vessels (20 internal carotid arteries and 7 common carotid arteries). Patients were followed with cerebral angiography, CT, sonography, or clinically for a mean of 14.6 months (range, 5 days to 48.2 months) with 17 of 26 patients having at least 6 months of follow-up. Procedural and long-term complication rates were calculated.
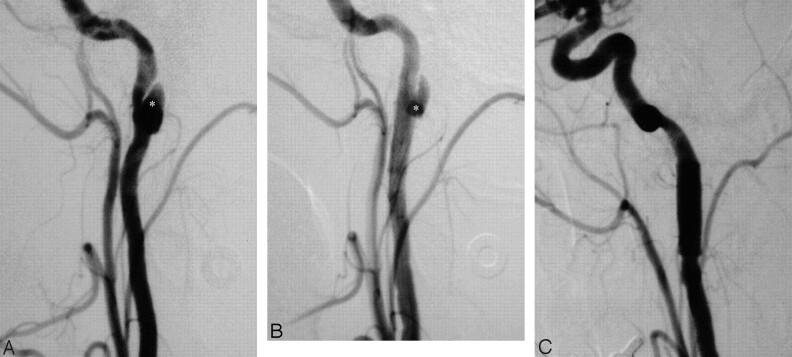
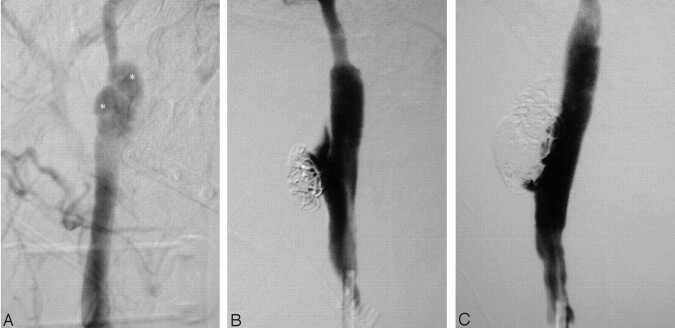
Results: Dissection-induced stenosis was reduced from 71 +/- 18% to no significant stenosis in 20 of the 21 patients with measurable stenosis. The procedural transient ischemic attack (TIA) rate was 3 of 29 procedures (10.3%). There were no procedural strokes. One patient required angioplasty of a common femoral artery. One procedure was terminated when an asymptomatic new intimal flap was created before intervention. Two patients had occlusions of the treated vessel noted at 22 days (presented with contralateral stroke) and 3.4 months (asymptomatic). There were 2 unrelated deaths from myocardial infarction at 8 days and 15.2 months. Two patients had recurrent ipsilateral TIA at 2.7 months and 12 months. The 30-day occlusion and death rate was 2 of 29 procedures (6.9%).
Conclusion: In this series, angioplasty and stent placement were effective in relieving stenosis secondary to carotid dissection with or without pseudoaneurysm and have low rates of ischemic complications.
Figures

Similar articles
-
Endovascular management of extracranial carotid artery dissection achieved using stent angioplasty.AJNR Am J Neuroradiol. 2000 Aug;21(7):1280-92. AJNR Am J Neuroradiol. 2000. PMID: 10954281 Free PMC article.
-
Long-term outcomes after carotid stent placement treatment of carotid artery dissection.Neurosurgery. 1999 Dec;45(6):1368-73; discussion 1373-4. doi: 10.1097/00006123-199912000-00022. Neurosurgery. 1999. PMID: 10598705
-
Percutaneous transluminal angioplasty and stent placement for recurrent carotid artery stenosis.J Neurosurg. 1999 Apr;90(4):688-94. doi: 10.3171/jns.1999.90.4.0688. J Neurosurg. 1999. PMID: 10193614
-
Long-term clinical and angiographic outcomes in patients with cervico-cranial dissections treated with stent placement: a meta-analysis of case series.J Neurotrauma. 2012 May 1;29(7):1342-53. doi: 10.1089/neu.2011.1963. Epub 2012 Feb 7. J Neurotrauma. 2012. PMID: 22188127 Review.
-
Endovascular stenting for the treatment of traumatic internal carotid injuries: expanding experience.J Trauma. 2008 Dec;65(6):1561-6. doi: 10.1097/TA.0b013e31817fd954. J Trauma. 2008. PMID: 19077655 Review.
Cited by
-
Reversal of carotid dissection-induced ocular and cerebral ischemia by stenting.Am J Ophthalmol Case Rep. 2017 May 18;7:50-54. doi: 10.1016/j.ajoc.2017.05.003. eCollection 2017 Sep. Am J Ophthalmol Case Rep. 2017. PMID: 29260078 Free PMC article.
-
Internal Carotid Artery Dissection - A Case for Antithrombotic Therapy in the Era of (Minimally) Invasive Procedures.Maedica (Bucur). 2020 Dec;15(4):536-542. doi: 10.26574/maedica.2020.15.4.536. Maedica (Bucur). 2020. PMID: 33603914 Free PMC article.
-
The role of neuroimaging in the latent period of blunt traumatic cerebrovascular injury.Open Neuroimag J. 2011;5:225-31. doi: 10.2174/1874440001105010225. Epub 2011 Dec 1. Open Neuroimag J. 2011. PMID: 22253664 Free PMC article.
-
Comprehensive analysis of intra-arterial treatment for acute ischemic stroke due to cervical artery dissection.J Neurointerv Surg. 2017 Jul;9(7):654-658. doi: 10.1136/neurintsurg-2016-012421. Epub 2016 Jun 10. J Neurointerv Surg. 2017. PMID: 27286992 Free PMC article.
-
Flow-diverter Stents for Internal Carotid Artery Reconstruction Following Spontaneous Dissection: A Technical Report.Clin Neuroradiol. 2019 Dec;29(4):707-715. doi: 10.1007/s00062-018-0707-z. Epub 2018 Aug 13. Clin Neuroradiol. 2019. PMID: 30105560
References
-
- Leys D, Lucas C, Gobert M, et al. Cervical artery dissections. Eur Neurol 1997;37:3–12 - PubMed
-
- Lucas C, Moulin T, Deplanque D, et al. Stroke patterns of internal carotid artery dissection in 40 patients. Stroke 1998;29:2646–2648 - PubMed
-
- Schievink WI. The treatment of spontaneous carotid and vertebral artery dissections. Curr Opin Cardiol 2000;15:316–321 - PubMed
-
- Brandt T, Caplan L. Spontaneous arterial dissection. Curr Treat Options Neurol 2001;3:463–469 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous