

Improving acceptance of computerized prescribing alerts in ambulatory care
- PMID: 16221941
- PMCID: PMC1380196
- DOI: 10.1197/jamia.M1868
Improving acceptance of computerized prescribing alerts in ambulatory care
Abstract
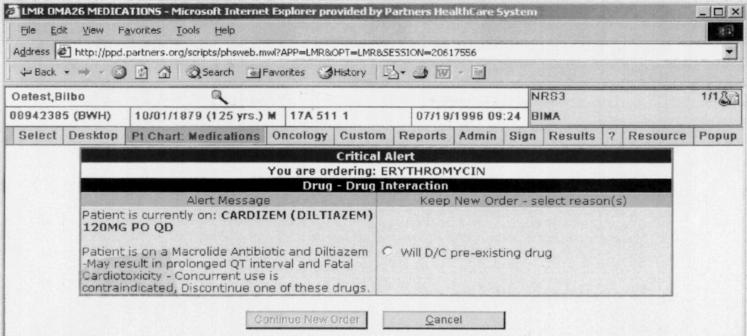
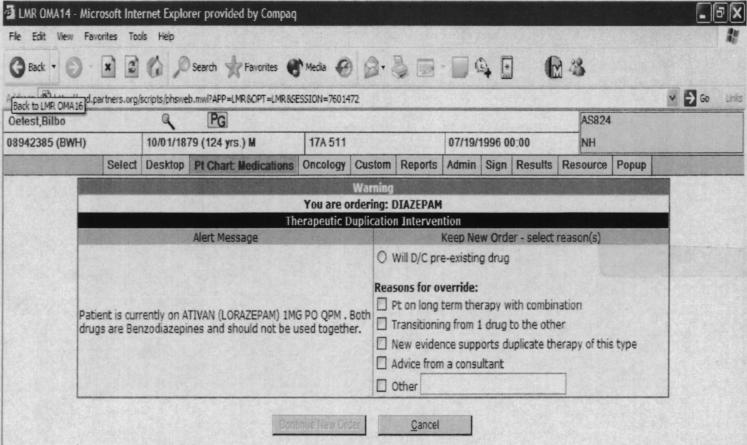
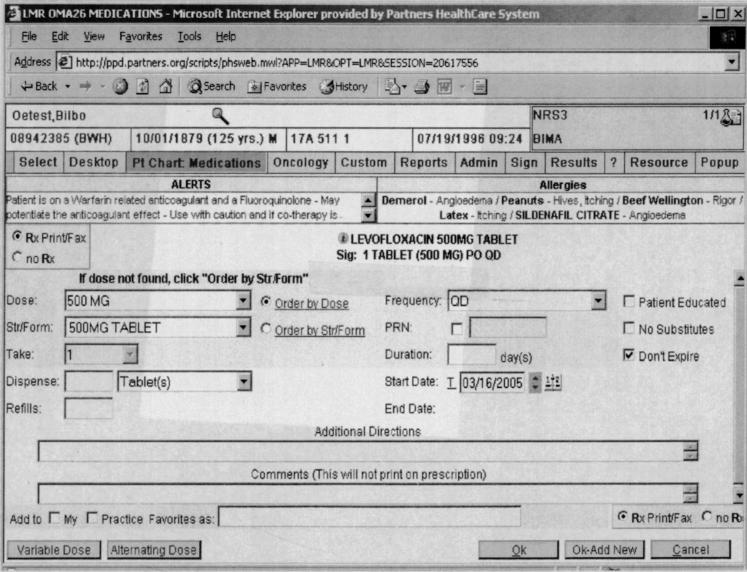
Computerized drug prescribing alerts can improve patient safety, but are often overridden because of poor specificity and alert overload. Our objective was to improve clinician acceptance of drug alerts by designing a selective set of drug alerts for the ambulatory care setting and minimizing workflow disruptions by designating only critical to high-severity alerts to be interruptive to clinician workflow. The alerts were presented to clinicians using computerized prescribing within an electronic medical record in 31 Boston-area practices. There were 18,115 drug alerts generated during our six-month study period. Of these, 12,933 (71%) were noninterruptive and 5,182 (29%) interruptive. Of the 5,182 interruptive alerts, 67% were accepted. Reasons for overrides varied for each drug alert category and provided potentially useful information for future alert improvement. These data suggest that it is possible to design computerized prescribing decision support with high rates of alert recommendation acceptance by clinicians.
Figures
References
-
- Bates DW, Leape LL, Cullen DJ, Laird N, Peterson LA, Teich JM, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998;280:1311–6. - PubMed
-
- Teich JM, Merchia PR, Schmiz JL, Kuperman GJ, Spurr CD, Bates DW. Effects of computerized physician order entry on prescribing practices. Arch Intern Med. 2000;160:2741–7. - PubMed
-
- Kuperman GJ, Teich JM, Gandhi TK, Bates DW. Patient safety and computerized medication ordering at Brigham and Women's Hospital. Jt Comm J Qual Improv. 2001;27:509–21. - PubMed
-
- Gandhi TK, Weingart SN, Seger AC, Seger DL, Boris J, Burdick E, et al. Impact of basic computerized prescribing on outpatient medication errors and adverse drug events. J Gen Intern Med. 2001;16(Suppl 1):195.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
