

A phase I trial of high-dose palliative radiotherapy plus concurrent weekly Vinorelbine and Cisplatin in patients with locally advanced and metastatic NSCLC
- PMID: 16222311
- PMCID: PMC2361626
- DOI: 10.1038/sj.bjc.6602759
A phase I trial of high-dose palliative radiotherapy plus concurrent weekly Vinorelbine and Cisplatin in patients with locally advanced and metastatic NSCLC
Abstract
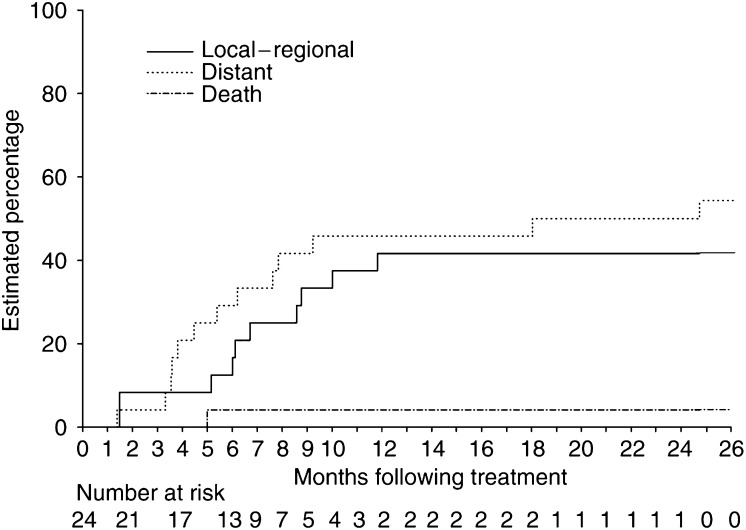
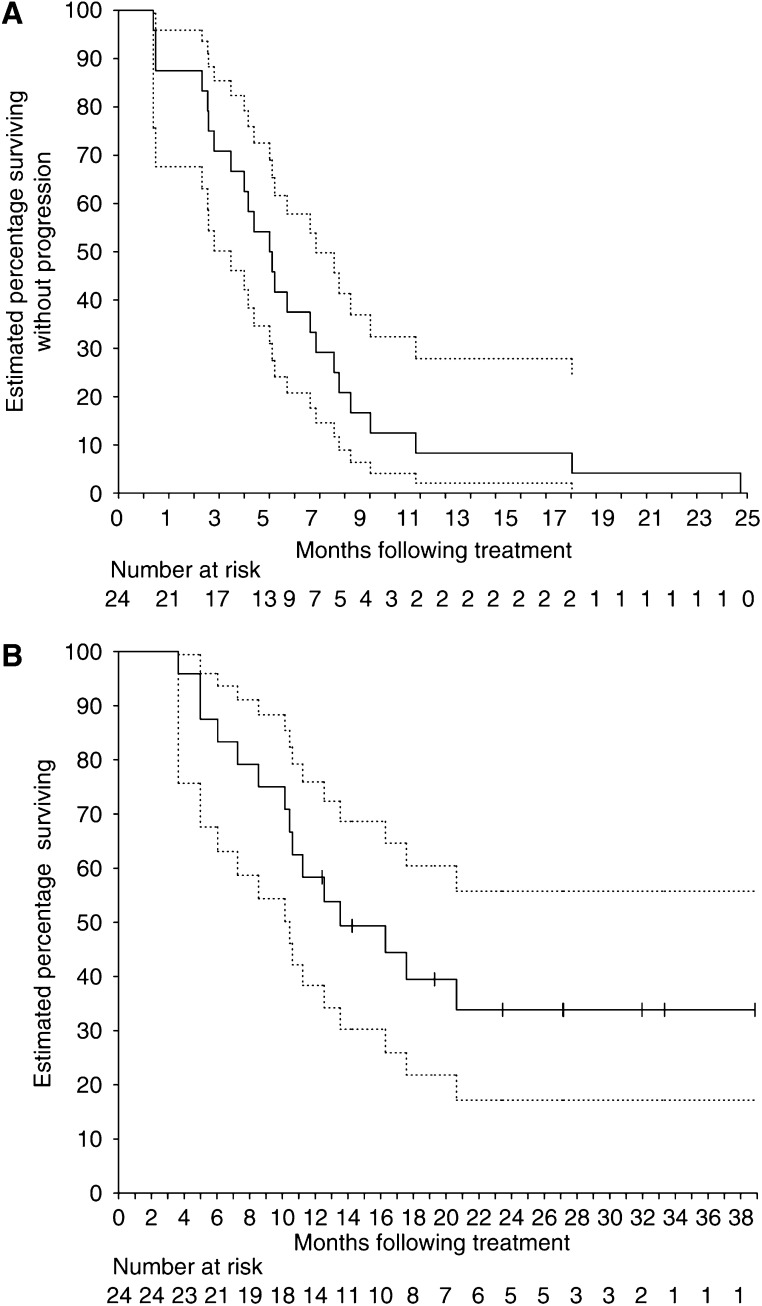
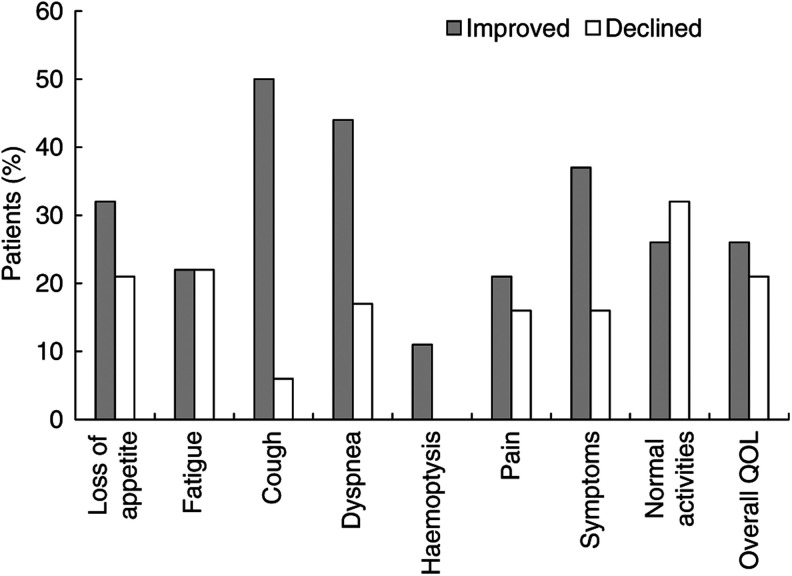
The role of concurrent chemoradiotherapy (CRT) in patients with non-small-cell lung cancer (NSCLC) unsuitable for radical therapy but who require locoregional treatment has not been defined. The aims of this phase I trial were thus to develop a novel regimen of weekly chemotherapy concurrent with high-dose palliative RT (40 Gy/20 fractions) and assess its tolerability, objective and symptomatic response rates. Eligible patients had stage I-IIIB NSCLC unsuitable for radical RT or limited stage IV disease, ECOG PS<or=1 and required locoregional therapy. Treatment was RT (40 Gy/20 fractions/5 per week) and weekly Vinorelbine plus Cisplatin escalated in six planned dose levels (DLs). At 4 weeks post-RT, patients received two cycles of Cisplatin 80 mg m-2 day 1+Vinorelbine 25 mg m-2 days 1, 8, 15. Dose-limiting toxicities (DLTs) were defined in the CRT phase. Disease-related symptoms were assessed by the Lung Cancer Symptom Scale. In all, 24 patients accrued, stage IIIB (n=12) and IV disease (n=10). The highest administered dose was at DL 4, Vinorelbine 30 mg m-2+Cisplatin 20 mg m-2 with DLTs of grade 4 neutropenia in two of three patients. No grade 3 or 4 nonhaematological toxicities were observed. The overall radiological response rate was 65% (n=23: complete response 4% and partial response 61%) and infield FDG-PET responses were seen in 89% (n=18). There was an improvement or stabilisation of symptoms and quality of life. Dose level 3, Vinorelbine 25 mg m-2+Cisplatin 20 mg m-2, is recommended for further assessment. This regimen was tolerable and produced meaningful responses for patients for whom locoregional control is required, but who are unsuitable for radical CRT.
Figures
References
-
- Abratt RP, Shepherd LJ, Salton DG (1995) Palliative radiation for stage 3 non-small cell lung cancer – a prospective study of two moderately high dose regimens. Lung Cancer 13: 137–143 - PubMed
-
- Anderson H, Hopwood P, Stephens RJ, Thatcher N, Cottier B, Nicholson M, Milroy R, Maughan TS, Falk SJ, Bond MG, Burt PA, Connolly CK, McIllmurray MB, Carmichael J (2000) Gemcitabine plus best supportive care (BSC) vs BSC in inoperable non-small cell lung cancer – a randomized trial with quality of life as the primary outcome. UK NSCLC Gemcitabine Group. Non-Small Cell Lung Cancer. Br J Cancer 83: 447–453 - PMC - PubMed
-
- Bezjak A, Dixon P, Brundage M, Tu D, Palmer MJ, Blood P, Grafton C, Lochrin C, Leong C, Mulroy L, Smith C, Wright J, Pater JL (2002) Randomized phase III trial of single vs fractionated thoracic radiation in the palliation of patients with lung cancer (NCIC CTG SC.15). Int J Radiat Oncol Biol Phys 54: 719–728 - PubMed
-
- Bogart JA (2004) Hypofractionated radiotherapy for advanced non-small-cell lung cancer: is the LINAC half full? J Clin Oncol 22: 765–768 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
