

Functional and morphological changes of the gut barrier during the restitution process after hemorrhagic shock
- PMID: 16222741
- PMCID: PMC4320358
- DOI: 10.3748/wjg.v11.i35.5485
Functional and morphological changes of the gut barrier during the restitution process after hemorrhagic shock
Abstract
Aim: To investigate the functional, morphological changes of the gut barrier during the restitution process after hemorrhagic shock, and the regional differences of the large intestine and small intestine in response to ischemia/reperfusion injury.
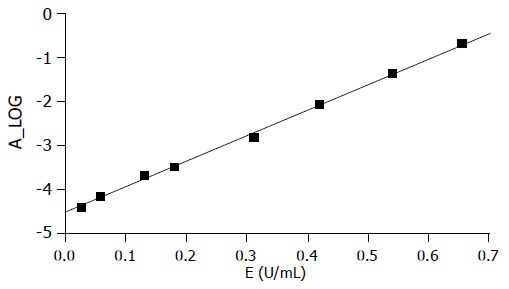
Methods: Forty-seven Sprague-Dawley rats with body weight of 250-300 g were divided into two groups: control group (sham shock n = 5) and experimental group (n = 42). Experimental group was further divided into six groups (n = 7 each) according to different time points after the hemorrhagic shock, including 0(th) h group, 1st h group, 3rd h group, 6th h group, 12th h group and 24th h group. All the rats were gavaged with 2 mL of suspension of lactulose (L) (100 mg/2 mL) and mannitol (M) (50 mg/each) at the beginning and then an experimental rat model of hemorrhagic shock was set up. The specimens from jejunum, ileum and colon tissues and the blood samples from the portal vein were taken at 0, 1, 3, 6, 12 and 24 h after shock resuscitation, respectively. The morphological changes of the intestinal mucosa, including the histology of intestinal mucosa, the thickness of mucosa, the height of villi, the index of mucosal damage and the numbers of goblet cells, were determined by light microscope and/or electron microscope. The concentrations of the bacterial endotoxin lipopolysaccharides (LPS) from the portal vein blood, which reflected the gut barrier function, were examined by using Limulus test. At the same time point, to evaluate intestinal permeability, all urine was collected and the concentrations of the metabolically inactive markers such as L and M in urine were measured by using GC-9A gas chromatographic instrument.
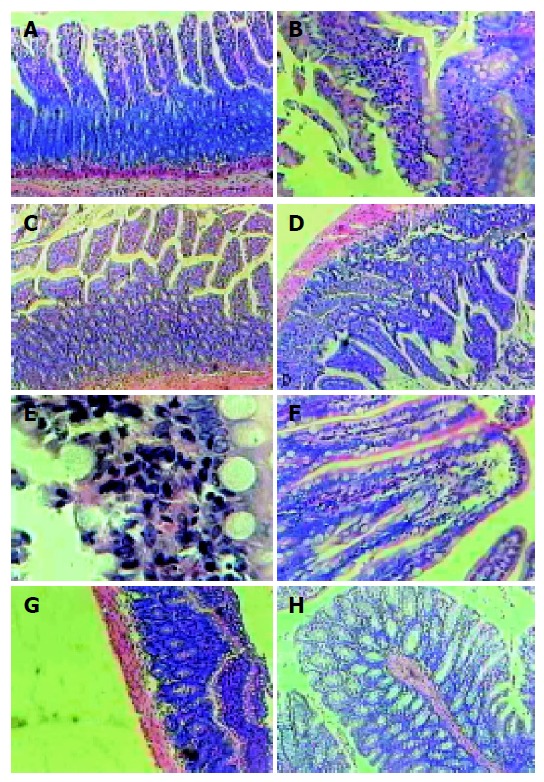
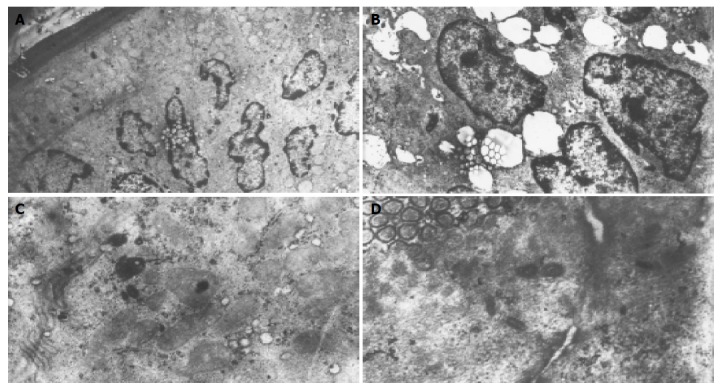
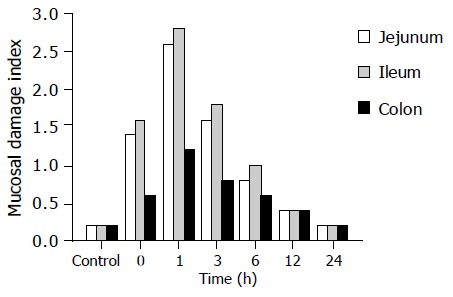
Results: After the hemorrhagic shock, the mucosal epithelial injury was obvious in small intestine even at the 0(th) h, and it became more serious at the 1st and the 3rd h. The tissue restitution was also found after 3 h, though the injury was still serious. Most of the injured mucosal restitution was established after 6 h and completed in 24 h. Two distinct models of cell death-apoptosis and necrosis-were involved in the destruction of rat intestinal epithelial cells. The number of goblet cells on intestinal mucosa was reduced significantly from 0 to 24 h (the number from 243+/-13 to 157+/-9 for ileum, 310+/-19 to 248+/-18 for colon; r = -0.910 and -0.437 respectively, all P<0.001), which was the same with the large intestine, but the grade of injury was lighter with the values of mucosal damage index in 3 h for jejunum, ileum, and colon being 2.8, 2.6, 1.2, respectively. The mucosal thickness and the height of villi in jejunum and ileum diminished in 1 h (the average height decreased from 309+/-24 to 204+/-23 microm and 271+/-31 to 231+/-28 microm, r = -0.758 and -0.659, all P<0.001; the thickness from 547+/-23 to 418+/-28 microm and 483+/-45 to 364+/-35 microm, r = -0.898 and -0.829, all P<0.001), but there was no statistical difference in the colon (F = 0.296, P = 0.934). Compared with control group, the urine L/M ratio and the blood LPS concentration in the experimental groups raised significantly, reaching the peak in 3-6 h (L/M: control vs 3 h vs 6 h was 0.029+/-0.09 vs 0.063+/-0.012 vs 0.078+/-0.021, r = -0.786, P<0.001; LPS: control vs 3 h vs 6 h was 0.09+/-0.021 vs 0.063+/-0.012 vs 0.25+/-0.023, r = -0.623, P<0.001), and it kept increasing in 24 h.
Conclusion: The gut barrier of the rats was seriously damaged at the early phase of ischemic reperfusion injury after hemorrhagic shock, which included the injury and atrophy in intestinal mucosa and the increasing of intestinal permeability. Simultaneously, the intestinal mucosa also showed its great repairing potentiality, such as the improvement of the intestinal permeability and the recovery of the morphology at different phases after ischemic reperfusion injury. The restitution of gut barrier function was obviously slower than that of the morphology and there was no direct correlation between them. Compared with the small intestine, the large intestine had stronger potentiality against injury. The reduction of the amount of intestinal goblet cells by injury did not influence the ability of intestinal mucosal restitution at a certain extent and it appeared to be intimately involved in the restitution of the epithelium.
Figures
References
-
- Wilmore DW, Smith RJ, O'Dwyer ST, Jacobs DO, Ziegler TR, Wang XD. The gut: a central organ after surgical stress. Surgery. 1988;104:917–923. - PubMed
-
- Deitch EA, Forsythe R, Anjaria D, Livingston DH, Lu Q, Xu DZ, Redl H. The role of lymph factors in lung injury, bone marrow suppression, and endothelial cell dysfunction in a primate model of trauma-hemorrhagic shock. Shock. 2004;22:221–228. - PubMed
-
- Davidson MT, Deitch EA, Lu Q, Osband A, Feketeova E, Németh ZH, Haskó G, Xu DZ. A study of the biologic activity of trauma-hemorrhagic shock mesenteric lymph over time and the relative role of cytokines. Surgery. 2004;136:32–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
