

Vaccines for tuberculosis: novel concepts and recent progress
- PMID: 16223953
- PMCID: PMC1265910
- DOI: 10.1128/CMR.18.4.687-702.2005
Vaccines for tuberculosis: novel concepts and recent progress
Abstract
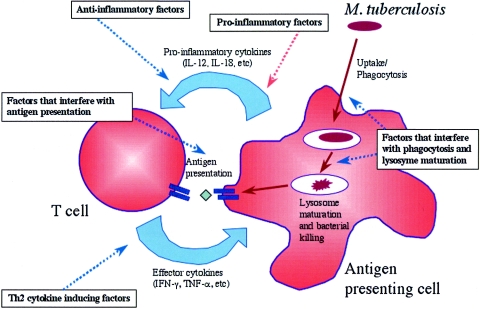
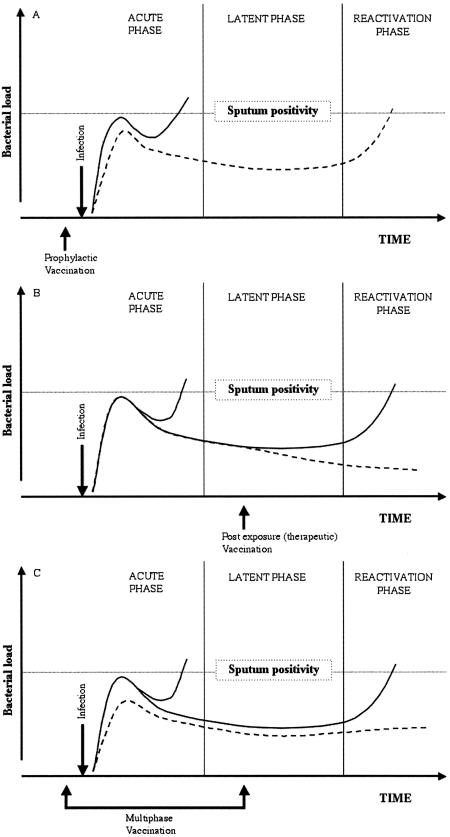
Three-quarters of a century after the introduction of Mycobacterium bovis BCG, the first tuberculosis vaccine, new vaccines for tuberculosis are finally entering clinical trials. This breakthrough is based not only on advances in proteomics and genomics which have made the construction of new vaccines possible, but also on a greatly expanded knowledge of the immunology of tuberculosis. Here we review our current understanding of how Mycobacterium tuberculosis subverts or survives the host's immune response to cause disease and why the current vaccination strategy, which relies on BCG, is only partially successful in countering the pathogen. This provides a background for describing the new generation of vaccines designed to supplement or replace the current vaccine and the different approaches they take to stimulate immunity against M. tuberculosis.
Figures
References
-
- Aaron, L., D. Saadoun, I. Calatroni, O. Launay, N. Memain, V. Vincent, G. Marchal, B. Dupont, O. Bouchaud, D. Valeyre, and O. Lortholary. 2004. Tuberculosis in HIV-infected patients: a comprehensive review. Clin. Microbiol. Infect. 10:388-398. - PubMed
-
- Agger, E. M., and P. Andersen. 2001. Tuberculosis subunit vaccine development: on the role of interferon-gamma. Vaccine 19:2298-2302. - PubMed
-
- Anonymous 1999. Fifteen year follow up of trial of BCG vaccines in south India for tuberculosis prevention. Indian J. Med. Res. 110:56-69. - PubMed
-
- Anonymous 2005. Global tuberculosis control - surveillance, planning, financing W.H.O./HTM/TB/2005. World Health Organization, Geneva, Switzerland.
-
- Arias, M., M. Rojas, J. Zabaleta, J. I. Rodriguez, S. C. Paris, L. F. Barrera, and L. F. Garcia. 1997. Inhibition of virulent Mycobacterium tuberculosis by Bcg(r) and Bcg(s) macrophages correlates with nitric oxide production. J Infect. Dis. 176:1552-1558. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
