

Rituximab for refractory Wegener's granulomatosis: report of a prospective, open-label pilot trial
- PMID: 16224107
- PMCID: PMC2662987
- DOI: 10.1164/rccm.200507-1144OC
Rituximab for refractory Wegener's granulomatosis: report of a prospective, open-label pilot trial
Abstract
Rationale: Standard therapy for Wegener's granulomatosis is fraught with substantial toxicity and not always effective. B lymphocytes have been implicated in the pathogenesis of Wegener's granulomatosis. Their depletion has been proposed as salvage therapy for refractory disease. Earlier encouraging reports are confounded by concomitant immunosuppressive medications and include only limited available biomarker data.
Objectives: To evaluate the efficacy and safety of rituximab for remission induction in refractory Wegener's granulomatosis.
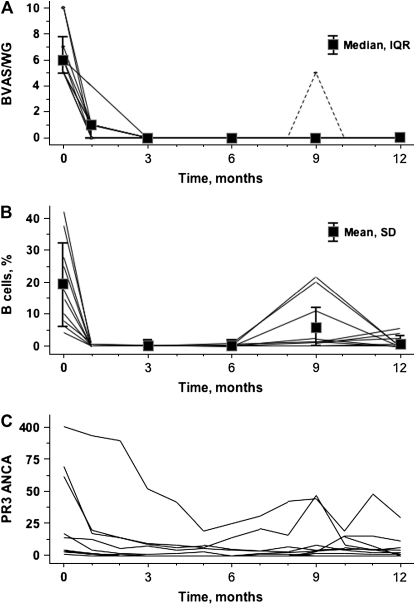
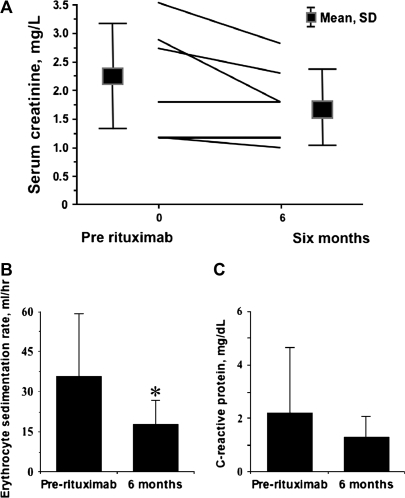
Methods: A prospective open-label pilot trial was conducted with 10 patients monitored for 1 yr. Included were patients with active severe antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis, ANCA positivity, and resistance to (or intolerance of) cyclophosphamide. The remission induction regimen consisted of oral prednisone (1 mg/kg/d) and four weekly infusions of rituximab (375 mg/m(2)). Prednisone was tapered and discontinued over 5 mo. Failure to achieve remission, a clinical flare in the absence of B lymphocytes, and inability to complete the glucocorticoid taper were considered treatment failures.
Main results: Three women and seven men (median age, 57 yr; range, 25-72 yr) were enrolled. All had ANCA reacting with proteinase-3. The median activity score at enrollment was 6 (range, 5-10). All patients tolerated rituximab well, achieved swift B-lymphocyte depletion and complete clinical remission (activity score, 0) by 3 mo, and were tapered off glucocorticoids by 6 mo. Five patients were retreated with rituximab alone for recurring/rising ANCA titers according to protocol. One patient experienced a clinical flare after B lymphocyte reconstitution.
Conclusion: In this cohort, rituximab was a well-tolerated and effective remission induction agent for severe refractory Wegener's granulomatosis.
Figures
Comment in
-
Rituximab in refractory Wegener's granulomatosis: Favorable or not?Am J Respir Crit Care Med. 2006 Apr 1;173(7):815-6; author reply 816. doi: 10.1164/ajrccm.173.7.815a. Am J Respir Crit Care Med. 2006. PMID: 16556703 No abstract available.
References
-
- Jennette JC, Falk RJ, Andrassy K, Bacon BA, Churg J, Gross WL, Hagen EC, Hoffmann GS, Hunder GG, Kallenberg CGM, et al. Nomenclature of systemic vasculitides: the proposal of an international consensus conference. Arthritis Rheum 1994;37:187–192. - PubMed
-
- Jayne D, Rasmussen N, Andrassy K, Bacon P, Cohen Tervaert JW, Dadoniene J, Ekstrand A, Gaskin G, Gregorini G, de Groot K, et al. A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies. N Engl J Med 2003;349:36–44. - PubMed
-
- WGET Research Group. Etanercept plus standard therapy for Wegener's granulomatosis. N Engl J Med 2005;352:351–361. - PubMed
-
- Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, Rottem M, Fauci AS. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 1992;116:488–498. - PubMed
-
- Reinhold-Keller E, Beuge N, Latza U, de Groot K, Rudert H, Nolle B, Heller M, Gross WL. An interdisciplinary approach to the care of patients with Wegener's granulomatosis: long-term outcome in 155 patients. Arthritis Rheum 2000;43:1021–1032. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
