

doi: 10.3201/eid1209.041344.
Potential impact of antiviral drug use during influenza pandemic
Affiliations
- PMID: 16229762
- PMCID: PMC3371825
- DOI: 10.3201/eid1209.041344
Item in Clipboard
Potential impact of antiviral drug use during influenza pandemic
Emerg Infect Dis.
2005 Sep.
Abstract
The recent spread of highly pathogenic strains of avian influenza has highlighted the threat posed by pandemic influenza. In the early phases of a pandemic, the only treatment available would be neuraminidase inhibitors, which many countries are considering stockpiling for pandemic use. We estimate the effect on hospitalization rates of using different antiviral stockpile sizes to treat infection. We estimate that stockpiles that cover 20%-25% of the population would be sufficient to treat most of the clinical cases and could lead to 50% to 77% reductions in hospitalizations. Substantial reductions in hospitalization could be achieved with smaller antiviral stockpiles if drugs are reserved for persons at high risk.
Figures
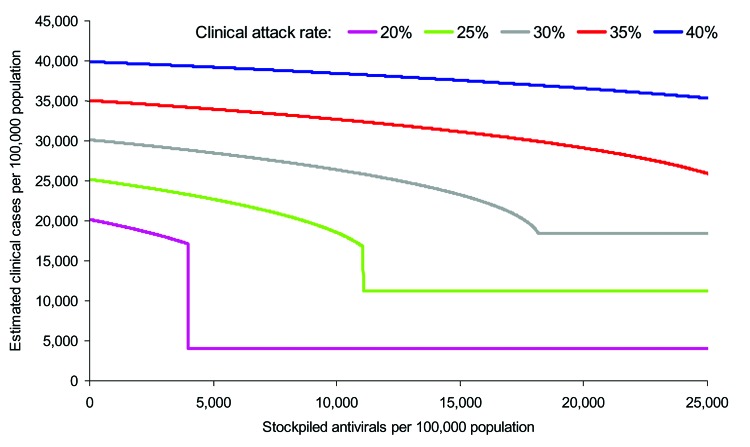
. Estimated impact of different sizes of antiviral stockpiles on the number of clinical cases at the end of the pandemic. Depicted are clinical attack rates before interventions of 20%, 25%, 30%, 35%, and 40%, with corresponding values for the basic reproduction number (R0) of 1.28, 1.39, 1.53, 1.72, and 2.0 respectively. The precipitous decreases observed with the 20% and 25% attack rates result at the points at which the stockpile becomes large enough to last long enough to prevent a recrudescence of the epidemic by suppressing the effective reproduction number.
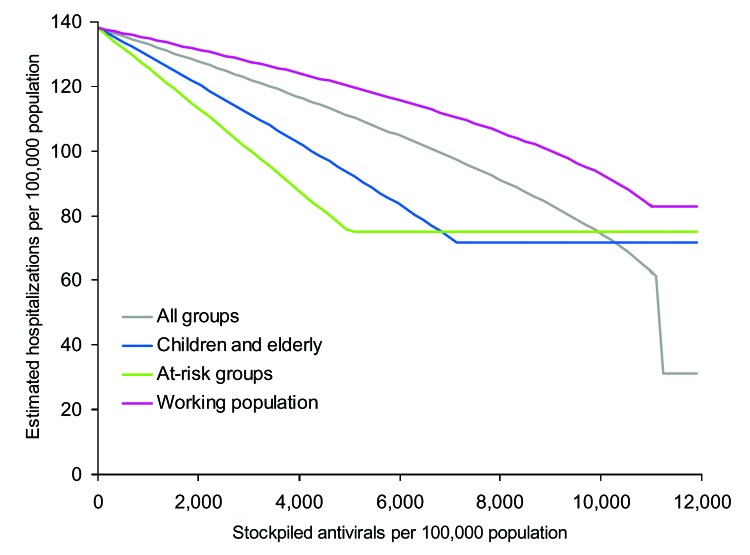
Estimated number of hospitalizations per 100,000 population when different antiviral treatment strategies are applied. Baseline scenario is when the clinical attack rate in the absence of interventions is 25% of the population.
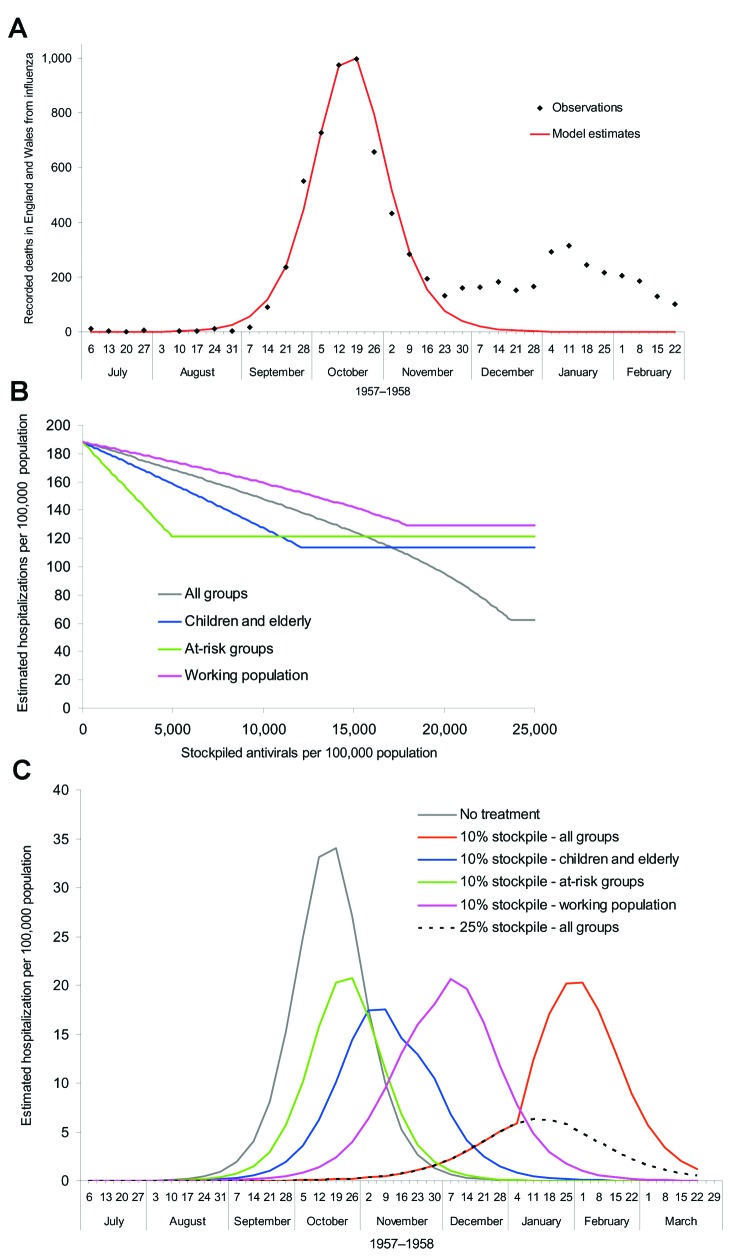
A), Output from the model fitted to the first wave of the 1957 pandemic scaled to fit observations from the 1957 pandemic (26). B), Estimated hospitalization rates from a simulated pandemic with available parameters from the 1957 pandemic, as influenced by stockpile size and treatment strategy. C), Impact of treatment strategy on the time course of hospitalizations when the stockpile size is fixed at 10% of the population, the stockpile is fixed at 25% of the population and all clinical cases are treated, and when no treatment is administered.
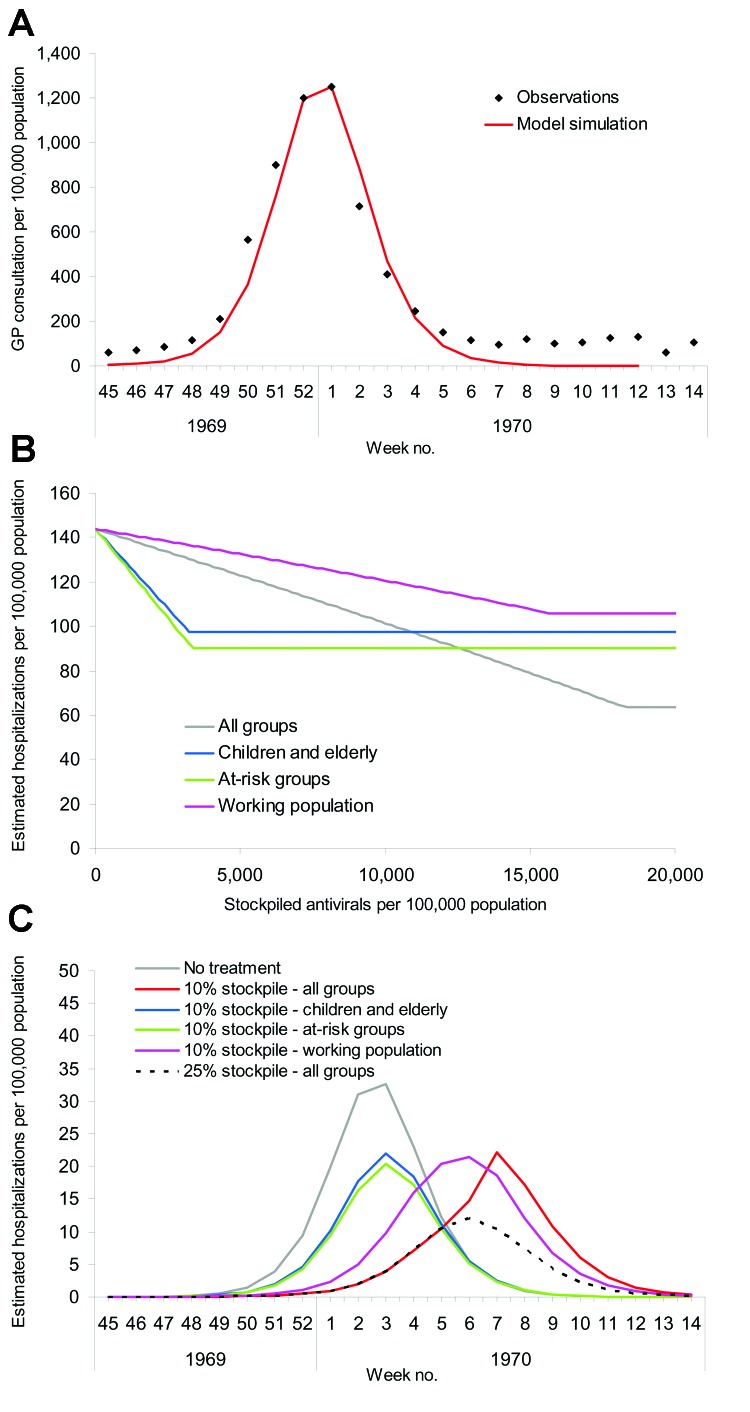
A), Output from the model fitted to the second wave of the 1968 pandemic scaled to fit observations from general practitioners (GPs) from the 1968 pandemic (29). B), Estimated hospitalization rates from a simulated pandemic with available parameters from the 1968 pandemic as influenced by stockpile size and treatment strategy. C), Impact of treatment strategy on the time course of hospitalizations when the stockpile size is fixed at 10% of the population, the stockpile is fixed at 25% of the population and all clinical cases are treated, and when no treatment is administered.
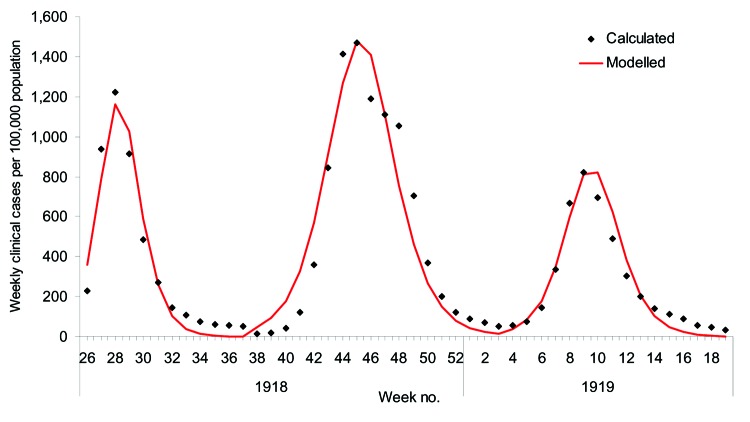
Clinical cases per week estimated by using the clinical case-fatality rates and weekly mortality statistics for the 1918 pandemic and by fitting the basic reproduction number (R0) to data from each of the waves by using the transmission model (28).
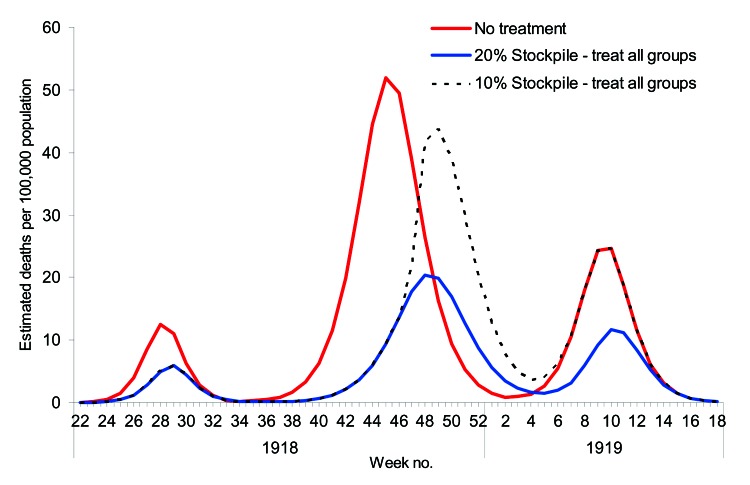
Estimated number of deaths from the 3 waves of the 1918 pandemic when there is no treatment, a 20% antiviral stockpile, and a 10% antiviral stockpile.
References
-
- World Health Organization. Influenza pandemic plan. The role of WHO and guidelines for national and regional planning. Geneva: The Organization; 1999.
-
- UK Department of Health. UK pandemic influenza contingency plan. March 2005. [cited 2005 Mar 1]. Available from http://www.dh.gov.uk/assetRoot/04/10/44/37/04104437.pdf
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical