

doi: 10.1136/hrt.2004.057182.
Coarctation of the aorta from fetus to adult: curable condition or life long disease process?
Affiliations
- PMID: 16230458
- PMCID: PMC1769162
- DOI: 10.1136/hrt.2004.057182
Item in Clipboard
Coarctation of the aorta from fetus to adult: curable condition or life long disease process?
Heart.
2005 Nov.
No abstract available
Figures
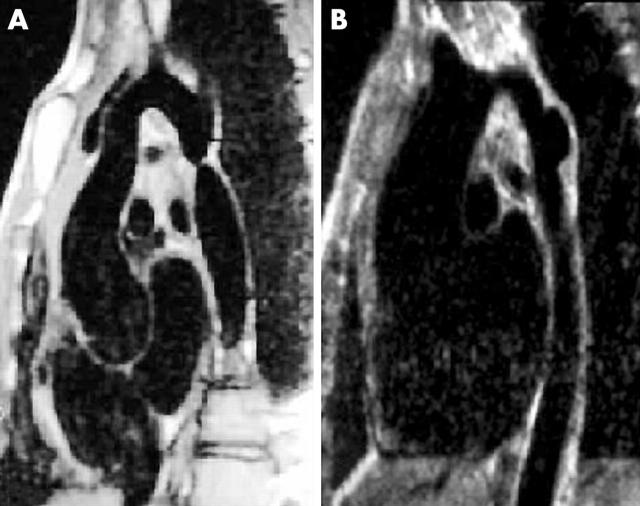
Magnetic resonance imaging scans of native coarctation in a 32 year old man (A) and aneurysm at balloon dilation site in a 14 year old boy (B).
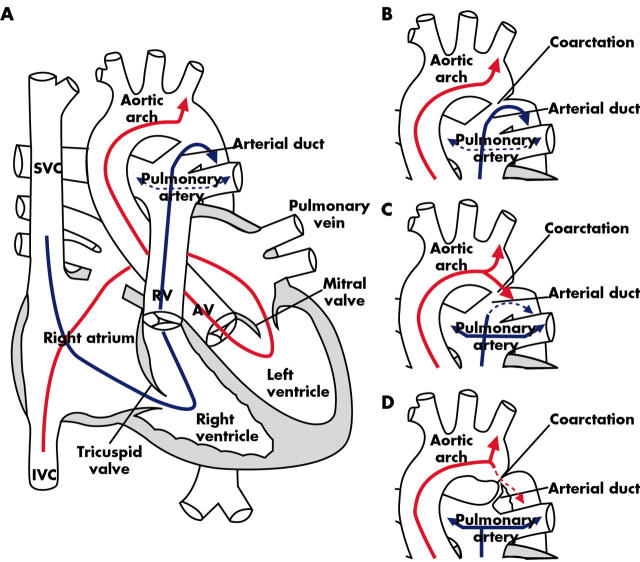
Diagram of normal fetal circulation. (A) Superior vena cava (SVC) blood flow (blue arrow) is directed through the tricuspid valve to the pulmonary artery and via the arterial duct to the lower body segment. Inferior vena cava (IVC) blood flow (red arrow) containing oxygenated blood from the placenta is directed across the foramen ovale to the left ventricle, ascending aorta and upper body segment with little flow across the isthmus between the left subclavian artery and the arterial duct. (B) Coarctation of the aorta in utero does not affect the fetal blood flow pattern. (C) After birth there is a fall in pulmonary resistance with increased pulmonary blood flow (blue arrows) and forward flow from the aortic arch to the descending aorta (red arrow). (D) As the duct constricts, the narrowing of the coarctation is accentuated and the increasing obstruction leads to a gradient (red dotted line).
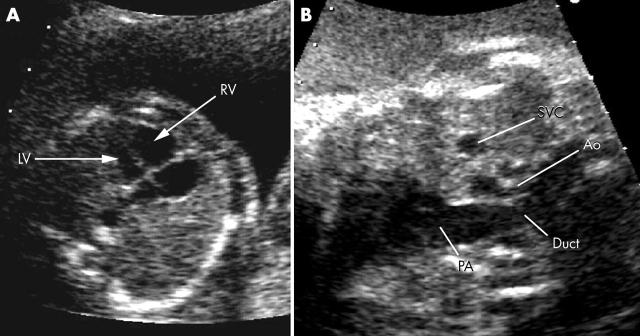
(A) Disproportion between the right and left ventricles is striking. (B) Great vessel disproportion between the aorta (Ao) and pulmonary artery (PA) is more specific for coarctation than ventricular disproportion. LV, left ventricle, RV, right ventricle; SVC, superior vena cava.
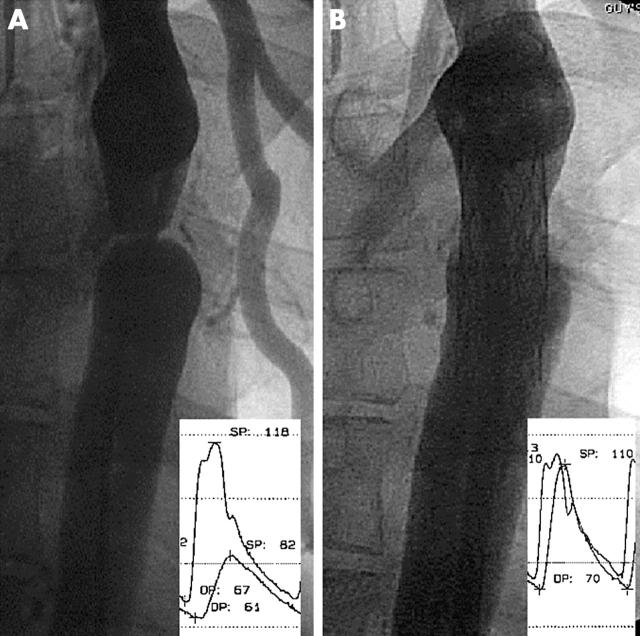
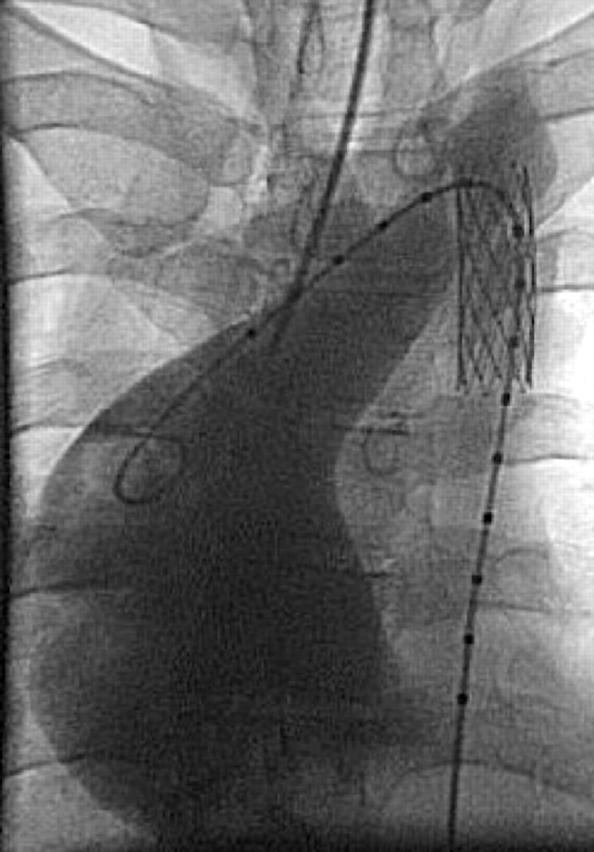
(A) Severe native coarctation in adult with large gradient and collateral vessels. (B) Stent implantation to 80% of the final aortic diameter abolishes the gradient.
Gross dilation of the ascending aorta (> 7 cm) in an adult patient with “mild” coarctation and a bicuspid aortic valve, followed for 20 years without treatment. Stent implantation has been performed before aortic root replacement.
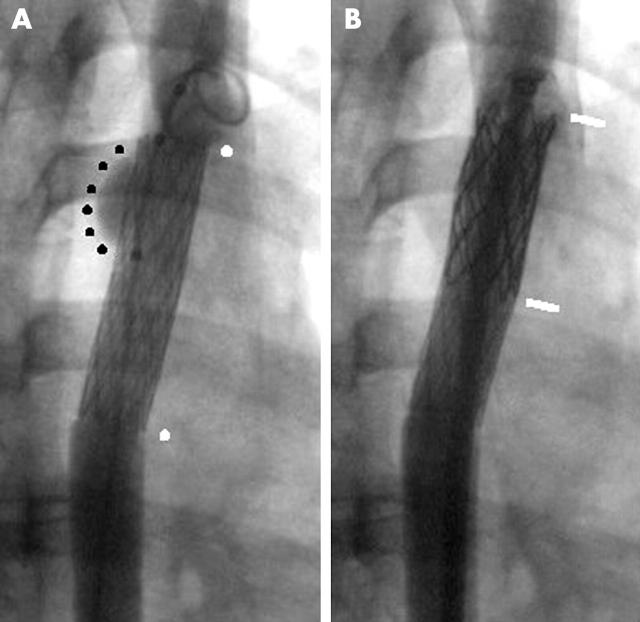
(A) Small aneurysm (black dots) at the top end of an uncovered stent (white dots) placed in a severe native coarctation presenting with an out of hospital cardiac arrest. (B) A covered stent (white lines) has been expanded inside the previous stent with exclusion of the aneurysm.
References
-
- Nielsen JC, Powell AJ, Gauvreau K, et al. Magnetic resonance imaging predictors of coarctation severity. Circulation 2005;111:622–8. ▸ Combination of MRI derived flow velocity and aortic narrowing indexed to body surface area predicts catheter gradients in excess of 20 mm Hg. - PubMed
-
- Vriend J, Zwinderman A, de Groot E, et al. Predictive value of mild, residual descending aortic narrowing for blood pressure and vascular damage in patients after repair of aortic coarctation. Eur Heart J 2005;26:84–90. ▸ Mild residual coarctation is associated with increased blood pressure and carotid intimal thickness. Should the threshold for intervention from current guidelines be lowered? - PubMed
-
- Head CEG, Jowett VC, Sharland GK, et al. Timing of presentation and postnatal outcome of infants suspected of having coarctation of the aorta during fetal life. Heart 2005;91:1070–4. ▸ Largest series of fetuses with suspected coarctation—the diagnosis was confirmed in one third postnatally. Coarctation was only detected late after duct closure in 7%. - PMC - PubMed
-
- Pfammatter JP, Ziemer G, Kaulitz R, et al. Isolated aortic coarctation in neonates and infants: results of resection and end-to-end anastomosis. Ann Thorac Surg 1996;62:778–82. ▸ Significant re-coarctation rate in neonates of 19%. - PubMed
-
- Younoszai AK, Reddy VM, Hanley FL, et al. Intermediate term follow-up of the end-to-side aortic anastomosis for coarctation of the aorta. Ann Thorac Surg 2002;74:1631–4. ▸ Recoarctation rate of only 5.5% by two years when performed in neonates—with good response to balloon dilation. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources