

The sensitivity and specificity of 0.5% apraclonidine in the diagnosis of oculosympathetic paresis
- PMID: 16234449
- PMCID: PMC1772929
- DOI: 10.1136/bjo.2005.074492
The sensitivity and specificity of 0.5% apraclonidine in the diagnosis of oculosympathetic paresis
Abstract
Aims: To evaluate the sensitivity and specificity of 0.5% apraclonidine test in the diagnosis of oculosympathetic paresis (OSP).
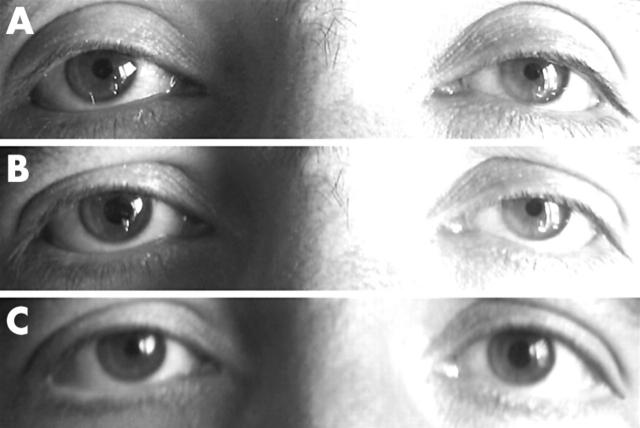
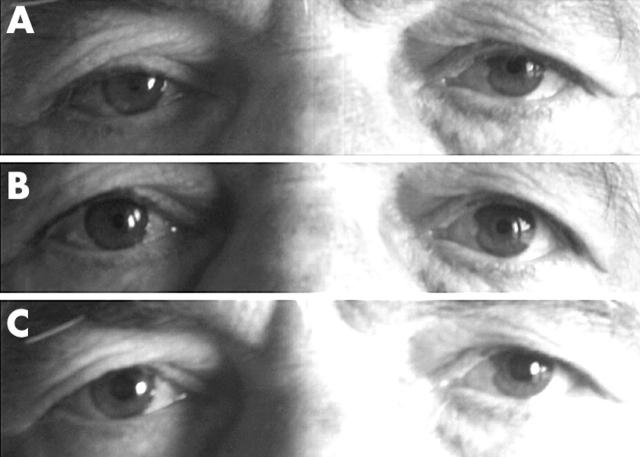
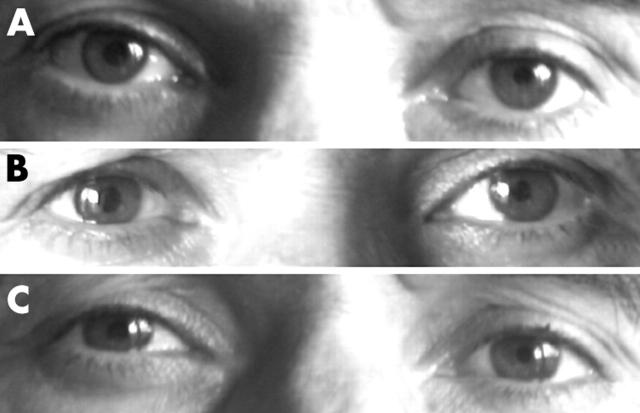
Method: Apraclonidine (0.5%) was administered to 31 eyes, nine with a diagnosis of Horner syndrome (HS), 22 with bilateral OSP caused by diabetes, and to 54 control eyes. All were confirmed with the cocaine test. The effects on pupil diameter and upper eyelid level were observed 1 hour later.
Results: Apraclonidine caused a mean dilation of 2.04 mm (range 1--4.5) (p<0.001) in the pupils with OSP and it caused pupillary constriction in the control eyes with a mean change of -0.14 mm (range 0.5 to --1) (p<0.05). It caused reversal of anisocoria in all HS cases. Its effects on both pupil diameters and upper lid levels differed significantly between the groups (p<0.001). The mean elevation in the upper lid was 1.75 mm (range 1--4) in the OSP group (p<0.001) and 0.61 mm (range 0--3) in the control group (p<0.001).
Conclusion: The effect of the apraclonidine (0.5%) test on the pupil diameter was diagnostic for OSP and had at least the same sensitivity and specificity as the cocaine test for the diagnosis of OSP.
Figures
Similar articles
-
False negative apraclonidine test in two patients with Horner syndrome.Klin Monbl Augenheilkd. 2008 May;225(5):520-2. doi: 10.1055/s-2008-1027349. Klin Monbl Augenheilkd. 2008. PMID: 18454417
-
Efficacy of apraclonidine 0.5% in the diagnosis of Horner syndrome in pediatric patients under low or high illumination.Am J Ophthalmol. 2006 Sep;142(3):469-74. doi: 10.1016/j.ajo.2006.04.052. Am J Ophthalmol. 2006. PMID: 16935593
-
Teaching NeuroImages: Positive apraclonidine test in Horner syndrome.Neurology. 2011 May 17;76(20):e100. doi: 10.1212/WNL.0b013e31821a4454. Neurology. 2011. PMID: 21576682 No abstract available.
-
Positive apraclonidine test 36 hours after acute onset of horner syndrome in dorsolateral pontomedullary stroke.J Neuroophthalmol. 2010 Mar;30(1):12-7. doi: 10.1097/WNO.0b013e3181b1b41f. J Neuroophthalmol. 2010. PMID: 20182200 Review.
-
[Acquired Horner's syndrome].Tidsskr Nor Laegeforen. 2011 May 20;131(9-10):950-4. doi: 10.4045/tidsskr.10.0935. Tidsskr Nor Laegeforen. 2011. PMID: 21606992 Review. Norwegian.
Cited by
-
Post-thyroidectomy iatrogenic Horner's syndrome with heterochromia.J Curr Ophthalmol. 2016 Mar 30;28(1):46-7. doi: 10.1016/j.joco.2016.02.004. eCollection 2016 Mar. J Curr Ophthalmol. 2016. PMID: 27239603 Free PMC article.
-
Efficacy of digital pupillometry for diagnosis of Horner syndrome.PLoS One. 2017 Jun 2;12(6):e0178361. doi: 10.1371/journal.pone.0178361. eCollection 2017. PLoS One. 2017. PMID: 28575101 Free PMC article.
-
Validation of Monocular Pupillometry in Healthy Controls and Patients With Autonomic Dysfunction: Pupillary Biomarkers for Autonomic Failure.Eur J Neurol. 2025 Aug;32(8):e70320. doi: 10.1111/ene.70320. Eur J Neurol. 2025. PMID: 40831073 Free PMC article.
-
14th EUNOS Congress: PORTO, PORTUGAL, 16-19 JUNE 2019.Neuroophthalmology. 2019 Jun 7;43(Suppl 1):1-221. doi: 10.1080/01658107.2019.1608780. eCollection 2019 Jun. Neuroophthalmology. 2019. PMID: 31528195 Free PMC article. No abstract available.
-
Safety of apraclonidine eye drops in diagnosis of Horner syndrome in an outpatient pediatric ophthalmology clinic.J AAPOS. 2021 Dec;25(6):336.e1-336.e4. doi: 10.1016/j.jaapos.2021.07.011. Epub 2021 Nov 2. J AAPOS. 2021. PMID: 34737082 Free PMC article.
References
-
- Zeitzer JM, Ayas NT, Wu AD, et al. Bilateral oculosympathetic paresis associated with loss of nocturnal melatonin secretion in patients with spinal cord injury. J Spinal Cord Med 2005;28:55–9. - PubMed
-
- Pittasch D, Lobmann R, Behrens-Baumann W, et al. Pupil signs of sympathetic autonomic neuropathy in patients with type 1 diabetes. Diabetes Care 2002;25:1545–50. - PubMed
-
- Toth C, Fletcher WA. Autonomic disorders and the eye. J Neuroophthalmol 2005;25:1–4. - PubMed
-
- Morales J, Brown SM, Abdul-Rahim AS, et al. Ocular effects of apraclonidine in Horner syndrome. Arch Ophthalmol 2000;118:951–4. - PubMed
-
- Bacal DA, Levy SR. The use of apraclonidine in the diagnosis of Horner syndrome in pediatric patients. Arch Ophthalmol 2004;122:276–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources