

Topical antibiotics without steroids for chronically discharging ears with underlying eardrum perforations
- PMID: 16235370
- PMCID: PMC6669264
- DOI: 10.1002/14651858.CD004618.pub2
Topical antibiotics without steroids for chronically discharging ears with underlying eardrum perforations
Abstract
Background: Chronic suppurative otitis media (CSOM) causes ear discharge and impairs hearing.
Objectives: Assess topical antibiotics (excluding steroids) for treating chronically discharging ears with underlying eardrum perforations (CSOM).
Search strategy: The Cochrane Ear, Nose and Throat Disorders Group Trials Register, the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library Issue 1, 2005), MEDLINE (January 1951 to March 2005), EMBASE (January 1974 to March 2005), LILACS (January 1982 to March 2005), AMED (1985 to March 2005), CINAHL (January 1982 to March 2005), OLDMEDLINE (January 1958 to December 1965), PREMEDLINE, metaRegister of Controlled Trials (mRCT), and article references.
Selection criteria: Randomised controlled trials; any topical antibiotic without steroids, versus no drug treatment, aural toilet, topical antiseptics, or other topical antibiotics excluding steroids; participants with CSOM.
Data collection and analysis: One author assessed eligibility and quality, extracted data, entered data onto RevMan; two authors inputted where there was ambiguity. We contacted investigators for clarifications.
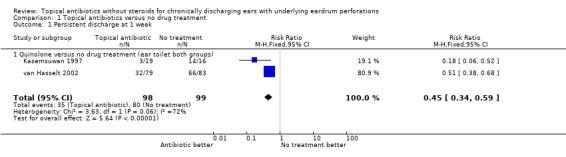
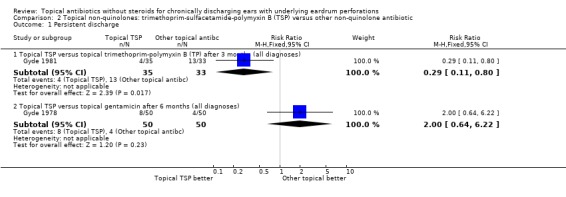
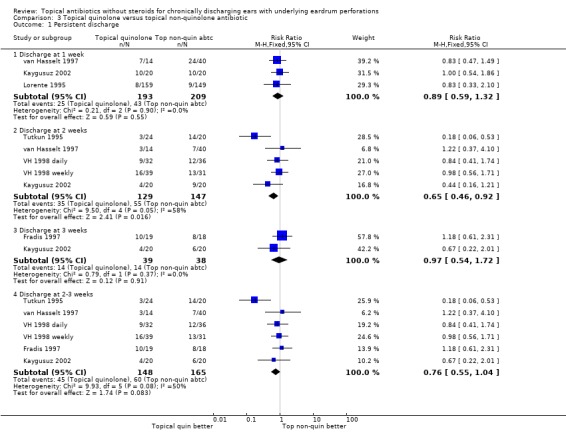
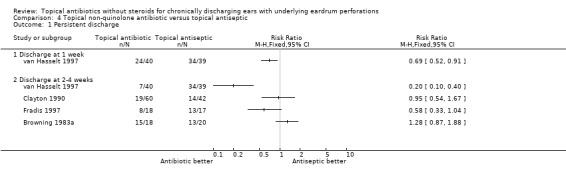
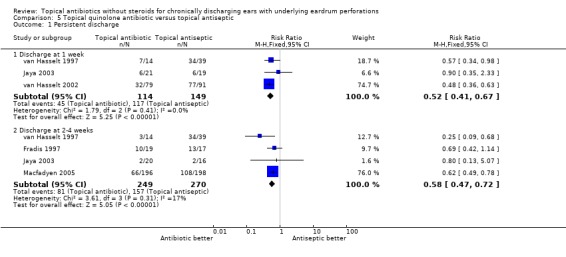
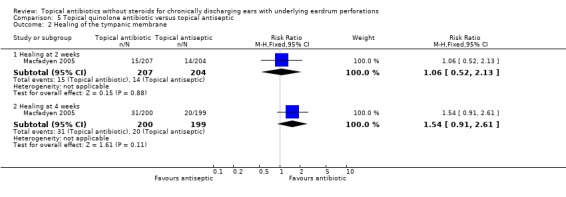
Main results: Fourteen trials (1,724 analysed participants or ears). CSOM definitions and severity varied; some included otitis externa, mastoid cavity infections and other diagnoses. Methodological quality varied; generally poorly reported, follow-up usually short, handling of bilateral disease inconsistent. Topical quinolone antibiotics were better than no drug treatment at clearing discharge at one week: relative risk (RR) was 0.45 (95% confidence interval (CI) 0.34 to 0.59) (two trials, N = 197). No statistically significant difference was found between quinolone and non-quinolone antibiotics (without steroids) at weeks one or three: pooled RR were 0.89 (95% CI 0.59 to 1.32) (three trials, N = 402), and 0.97 (0.54 to 1.72) (two trials, N = 77), respectively. A positive trend in favour of quinolones seen at two weeks was largely due to one trial and not significant after accounting for heterogeneity: pooled RR 0.65 (0.46 to 0.92) (four trials, N = 276) using the fixed-effect model, and 0.64 (95% CI 0.35 to 1.17) accounting for heterogeneity with the random-effects model. Topical quinolones were significantly better at curing CSOM than antiseptics: RR 0.52 (95% CI 0.41 to 0.67) at one week (three trials, N = 263), and 0.58 (0.47 to 0.72) at two to four weeks (four trials, N = 519). Meanwhile, non-quinolone antibiotics (without steroids) compared to antiseptics were more mixed, changing over time (four trials, N = 254). Evidence regarding safety was generally weak.
Authors' conclusions: Topical quinolone antibiotics can clear aural discharge better than no drug treatment or topical antiseptics; non-quinolone antibiotic effects (without steroids) versus no drug or antiseptics are less clear. Studies were also inconclusive regarding any differences between quinolone and non-quinolone antibiotics, although indirect comparisons suggest a benefit of topical quinolones cannot be ruled out. Further trials should clarify non-quinolone antibiotic effects, assess longer-term outcomes (for resolution, healing, hearing, or complications) and include further safety assessments, particularly to clarify the risks of ototoxicity and whether quinolones may result in fewer adverse events than other topical treatments.
Conflict of interest statement
None known. However, Carolyn Macfadyen and Carrol Gamble conducted and analysed a trial comparing a topical aural antiseptic, boric acid, with a topical aural antibiotic, ciprofloxacin (Macfadyen 2005).
Figures
Update of
References
References to studies included in this review
-
- Clayton MI, Osborne JE, Rutherford D, Rivron RP. A double‐blind, randomized, prospective trial of a topical antiseptic versus a topical antibiotic in the treatment of otorrhea. Clinical Otolaryngology and Allied Sciences 1990 Feb;15(1):7‐10. - PubMed
-
- Fradis M, Brodsky A, Ben‐David J, Srugo I, Larboni J, Podoshin L. Chronic otitis media treated topically with ciprofloxacin or tobramycin. Archives of Otolaryngology ‐ Head and Neck Surgery 1997 Oct;123(10):1057‐60. - PubMed
- Podoshin L, Brodzki A, Fradis M, Ben‐David J, Larboni J, Srugo I. [Local treatment of purulent chronic otitis media with ciprofloxacin]. Harefuah 1998 Jan 1;134(1):32‐6, 78. Hebrew. - PubMed
-
- Gyde MC, Randall RF. Double‐blind comparative study of trimethroprim‐sulphacetamide‐polymyxin b and gentamicin in the treatment of otorrhoea (author's transl) [Etude comparative a double insu de la trimethoprime‐sulfacetamide‐polymyxine B et de la gentamicine dans le traitement de l'otorrhée]. Annales d'Oto‐laryngologie et de Chirurgie Cervico‐faciale 1978 Jan‐Feb;95(1‐2):43‐55. - PubMed
-
- Gyde MC. A double‐blind comparative study of trimethoprim‐polymyxin B versus trimethoprim‐sulfacetamide‐polymyxin B otic solutions in the treatment of otorrhea. Journal of Laryngology and Otology 1981 Mar;95(3):251‐9. - PubMed
- Gyde MC. [Double‐blind comparative trial of trimethoprim‐polymyxin B and trimethoprim‐sulphacetamide‐polymyxin B ear drops in the treatment of otorrhoea (author's transl)]. Annales d' Oto‐Laryngologie et de Chirurgie Cervico‐Faciale 1981;98(1‐2):37‐40. French. - PubMed
References to studies excluded from this review
-
- Adler M, McDonald PJ, Trostmann U, Keyserling C, Tack K. Cefdinir vs. amoxicillin/clavulanic acid in the treatment of suppurative acute otitis media in children. Pediatric Infectious Disease Journal 2000 Dec;19(12 Suppl):S166‐70. - PubMed
-
- Akisada T, Orita Y, Sato Y, Handa T, Yoshihiro T, Kawai A, Urabe Y, Aihara T, Mori Y. [Clinical evaluation of Sairei‐to to chronic otitis media and cholesteatomas after tympanoplasty]. Practica Otologica 1997;92(Supplement):55‐60. Japanese.
- Akisada T, Orita Y, Yoshihiro T, Kawai A, Urabe Y, Take K, Okumoto K, Hidaka T, Aihara T, Hirai S. [Clinical evaluation of Sairei‐to for chronic otitis media and cholesteatoma after a tympanoplasty: Part II]. Practica Otologica 1998;98(Supplement):44‐8. Japanese.
-
- Anonymous. Local treatment with a corticosteroid‐antibiotic preparation in infections of the ear. The Practitioner 1970;205(229):691‐5. - PubMed
-
- Anonymous. Local treatment with a corticosteroid‐antibiotic preparation in infections of the ear. The Practitioner 1970;205(229):691‐5. - PubMed
-
- Arguedas A, Loaiza C, Herrera JF, Mohs E. Antimicrobial therapy for children with chronic suppurative otitis media without cholesteatoma. Pediatric Infectious Disease Journal 1994 Oct;13(10):878‐82. - PubMed
- Arguedas AG, Herrera JF, Faingezicht I, Mohs E. Ceftazidime for therapy of children with chronic suppurative otitis media without cholesteatoma. Pediatric Infectious Disease Journal 1993 Mar;12(3):246‐8. - PubMed
References to studies awaiting assessment
-
- Andersen JB. Otitis media and antibiotics [Otitis media of antibiotika]. Ugeskrift for Laeger 2002 Aug 12;164(33):3876‐7. - PubMed
-
- Iarlykov SA, Poliakova SD, Zemskov AM. [Correction of immunologic disorders in patients with chronic suppurative otitis media]. Vestnik Otorinolaringologii 1995 Jan‐Feb;95(1):9‐11. Russian. - PubMed
-
- Khakimov AM, Arifov SS, Faizulaeva FN. Effectiveness of antioxidant therapy of acute and chronic otitis media purulenta. Vestnik Otorinolaringologii 97;5:16‐9. - PubMed
-
- McKelvie P, Johnstone I, Jamieson I, Brooks C. The effect of gentamycin ear drops on the cochlea. British Journal of Audiology 1975;9(2):45‐7.
-
- Nawasreh O, Fraihat A. Topical ciprofloxacin versus topical gentamicin for chronic otitis media. Eastern Mediterranean Health Journal 2001 Jan‐Mar;7(1‐2):26‐30. - PubMed
Additional references
-
- Acuin J, Smith A, Mackenzie I. Interventions for chronic suppurative otitis media. The Cochrane Library 1998, Issue 2.
-
- Acuin J. Chronic suppurative otitis media. Clinical Evidence 2004 Dec;12:710‐29. - PubMed
-
- Barnett ED, Klein JO, Pelton SI, Luginbuhl LM. Otitis media in children born to human immunodeficiency virus‐infected mothers. Pediatric Infectious Disease Journal 1992 May;11(5):360‐4. - PubMed
-
- Berman S. Otitis media in developing countries. Pediatrics 1995 Jul;96(1 Pt 1):126‐31. - PubMed
-
- Bluestone CD, Klein JO. Chapter 24. Intratemporal Complications and Sequelae of Otitis Media. In: Bluestone CD, Stool SE, Kenna MA editor(s). Pediatric Otolaryngology. Third Edition. Vol. 1, London: WB Saunders Company, 1996:583‐635.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical