

Pharmacokinetics of insulin aspart in obesity, renal impairment, or hepatic impairment
- PMID: 16236036
- PMCID: PMC1884947
- DOI: 10.1111/j.1365-2125.2005.02476.x
Pharmacokinetics of insulin aspart in obesity, renal impairment, or hepatic impairment
Abstract
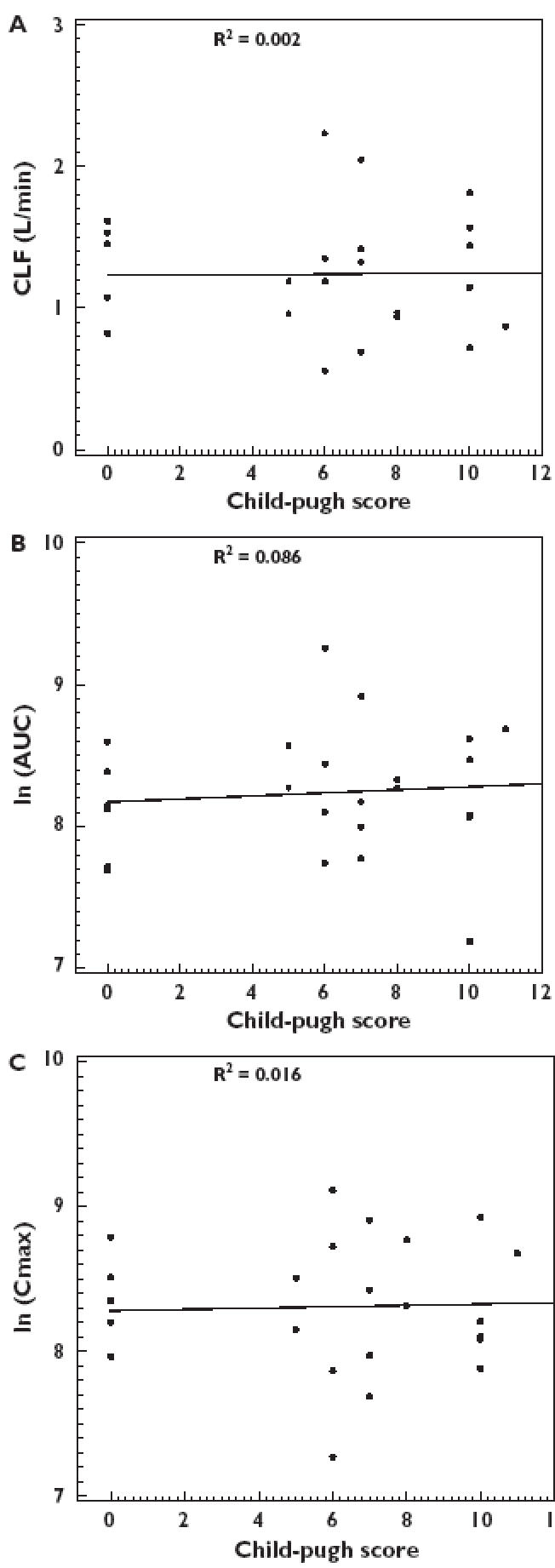
Aims: To assess the effects of body mass index, renal impairment (creatinine clearance), and hepatic impairment (Child-Pugh Score) on the pharmacokinetics of insulin aspart.
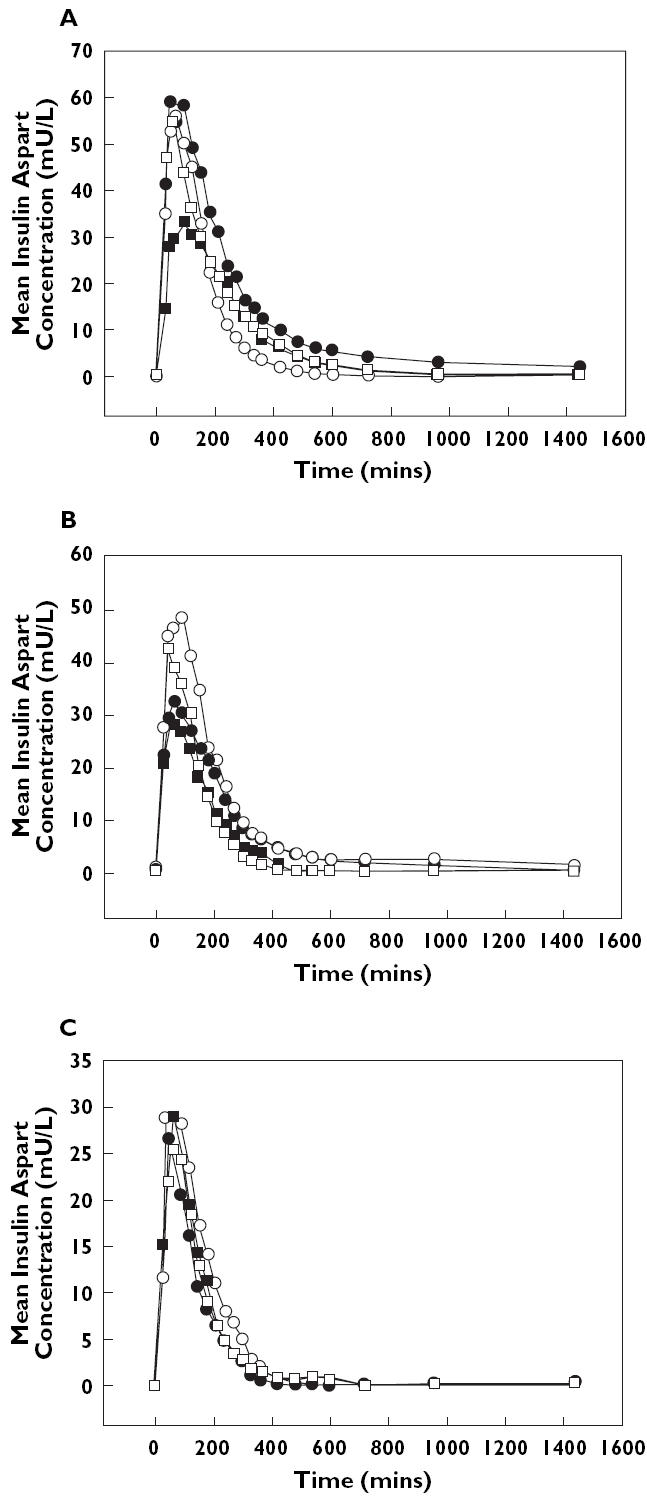
Methods: Pharmacokinetics of insulin aspart (injected subcutaneously in the abdomen immediately before a Boost standardized meal) were characterized in: (1) diabetic subjects with four ranges of BMI values (n = 23); (2) diabetic subjects with varying degrees of renal impairment (normal, n = 6 vs. two ranges of impairment, n = 12); and (3) nondiabetic patients with varying degrees of hepatic impairment (normal, n = 6 vs. three ranges of impairment, n = 18).
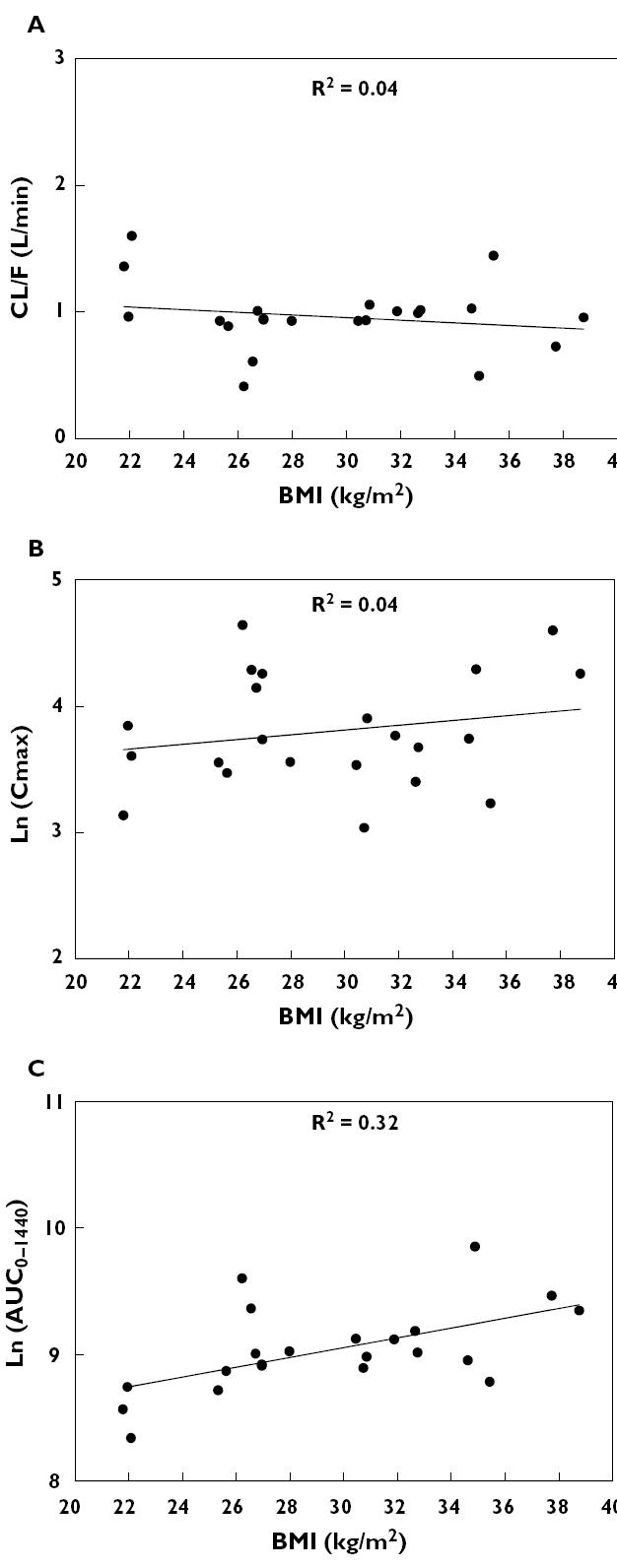
Results: There was no correlation between any pharmacokinetic variable and the degree of renal or hepatic impairment. Increasing obesity was associated with a decreased apparent clearance per kg body weight (beta = -0.0005, SE = 0.0001; P = 0.002), an increased t((1/2)) (beta = 3.513, SE = 1.636; P = 0.044), and an increased ln(AUC(0-360)) and ln(AUC(0-1440)) (beta = 0.030, SE = 0.013; P = 0.032 and beta = 0.039, SE = 0.0132; P = 0.006, respectively). However, obesity-related changes were smaller than individual variations in parameters.
Conclusions: Renal impairment, hepatic impairment, or BMI do not affect the pharmacokinetics of insulin aspart in a clinically significant manner.
Figures
References
-
- Setter SM, Corbett CF, Campbell RK, White JR. Insulin aspart: a new rapid-acting insulin analog. Ann Pharmacother. 2000;34(12):1423–31. - PubMed
-
- Clauson PG, Linde B. Absorption of rapid acting insulin in obese and non-obese NIDDM subjects. Diabetes Care. 1995;18:986–91. - PubMed
-
- Foss MC, Gouveia LMFB, Moyses Neto M, Paccola GM, Piccinato CE. Effect of hemodialysis on peripheral glucose metabolism of patients with chronic renal failure. Nephron. 1996;73:48–53. - PubMed
-
- Fliser D, Pacini G, Engerleither R, Kautzky-Willer A, Prager R, Franek E, Ritz E. Insulin resistance and hyperinsulinemia are already present in patients with incipient renal disease. Kidney Intl. 1998;53:343–1347. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
