

Classification of stillbirth by relevant condition at death (ReCoDe): population based cohort study
- PMID: 16236774
- PMCID: PMC1283273
- DOI: 10.1136/bmj.38629.587639.7C
Classification of stillbirth by relevant condition at death (ReCoDe): population based cohort study
Abstract
Objective: To develop and test a new classification system for stillbirths to help improve understanding of the main causes and conditions associated with fetal death.
Design: Population based cohort study.
Setting: West Midlands region.
Subjects: 2625 stillbirths from 1997 to 2003.
Main outcome measures: Categories of death according to conventional classification methods and a newly developed system (ReCoDe, relevant condition at death).
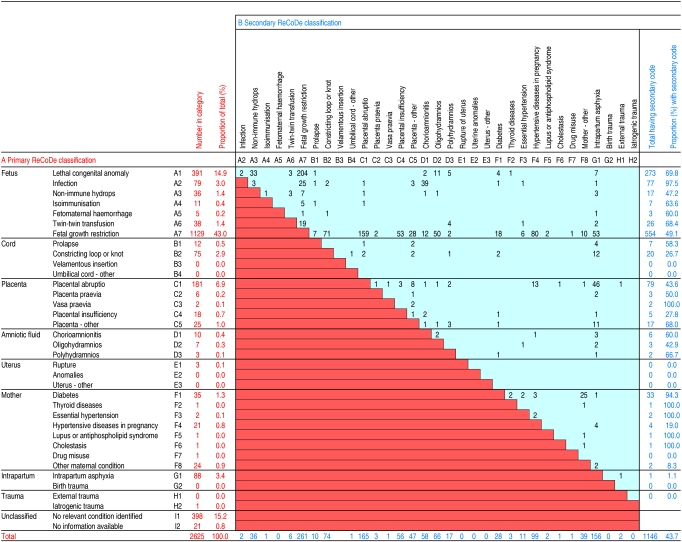
Results: By the conventional Wigglesworth classification, 66.2% of the stillbirths (1738 of 2625) were unexplained. The median gestational age of the unexplained group was 237 days, significantly higher than the stillbirths in the other categories (210 days; P < 0.001). The proportion of stillbirths that were unexplained was high regardless of whether a postmortem examination had been carried out or not (67% and 65%; P = 0.3). By the ReCoDe classification, the most common condition was fetal growth restriction (43.0%), and only 15.2% of stillbirths remained unexplained. ReCoDe identified 57.7% of the Wigglesworth unexplained stillbirths as growth restricted. The size of the category for intrapartum asphyxia was reduced from 11.7% (Wigglesworth) to 3.4% (ReCoDe).
Conclusion: The new ReCoDe classification system reduces the predominance of stillbirths currently categorised as unexplained. Fetal growth restriction is a common antecedent of stillbirth, but its high prevalence is hidden by current classification systems. This finding has profound implications for maternity services, and raises the question whether some hitherto "unexplained" stillbirths may be avoidable.
Figures
Comment in
-
Classification of stillbirth: cause, condition, or mechanism?BMJ. 2005 Nov 26;331(7527):1269-70; author reply 1270. doi: 10.1136/bmj.331.7527.1269-d. BMJ. 2005. PMID: 16308396 Free PMC article. No abstract available.
-
Classification of stillbirth: reclassification obscures things.BMJ. 2005 Nov 26;331(7527):1269; author reply 1270. doi: 10.1136/bmj.331.7527.1269-c. BMJ. 2005. PMID: 16308397 Free PMC article. No abstract available.
-
Classification of stillbirth: classification is not explanation.BMJ. 2005 Nov 26;331(7527):1269; author reply 1270. doi: 10.1136/bmj.331.7527.1269-b. BMJ. 2005. PMID: 16308398 Free PMC article. No abstract available.
References
-
- Maternal and Child Health Consortium. CESDI 8th annual report: Confidential Enquiry of Stillbirths and Deaths in Infancy, London 2001.
-
- Wigglesworth JS. Monitoring perinatal mortality—a pathophysiological approach. Lancet 1980;Sep 27: 684-7. - PubMed
-
- Hey EN, LLoyd DJ, Wigglesworth JS. Classifying perinatal death: fetal and neonatal factors. Br J Obstet Gynaecol 1986;93: 1213-23. - PubMed
-
- Cole SK, Hey EN, Thomson AM. Classifying perinatal death: an obstetric approach. Br J Obstet Gynaecol 1986;93: 1204-12. - PubMed
-
- Gardosi J, Chang A, Kalyan B, Sahota D, Symonds EM. Customised antenatal growth charts. Lancet 1992;339: 283-7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical