

The 1-year impact of severe acute respiratory syndrome on pulmonary function, exercise capacity, and quality of life in a cohort of survivors
- PMID: 16236881
- PMCID: PMC7094276
- DOI: 10.1378/chest.128.4.2247
The 1-year impact of severe acute respiratory syndrome on pulmonary function, exercise capacity, and quality of life in a cohort of survivors
Abstract
Objective: To examine pulmonary function, exercise capacity, and health-related quality of life (HRQoL) among severe acute respiratory syndrome (SARS) survivors.
Methods: We evaluated survivors with confirmed SARS at the Prince of Wales Hospital, Hong Kong, at 3, 6, and 12 months after symptom onset. Our assessment included: lung volume (total lung capacity [TLC], vital capacity, residual volume, functional residual capacity), spirometry (FVC, FEV1), diffusing capacity of the lung for carbon monoxide (D(LCO)), inspiratory and expiratory respiratory muscle strength, 6-min walk distance (6MWD), chest radiographs (CXRs), and HRQoL by Medical Outcomes Study 36-Item Short-Form General Health Survey questionnaire.
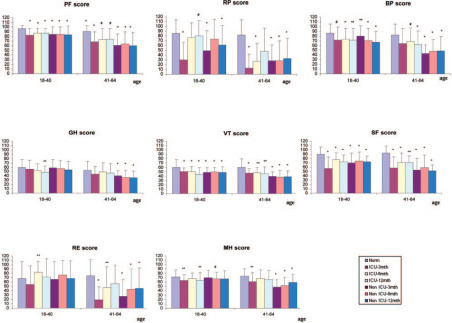
Results: Ninety-seven patients completed the serial assessments. There were 39 male and 58 female patients, and 63 patients (70%) were health-care workers (mean age, 36.9 years [SD, 9.5 years]; body mass index, 23.7 kg/m2 [SD, 4.0 kg/m2]). At 1 year, 27 patients (27.8%) had abnormal CXR findings. Four patients (4.1%), 5 patients (5.2%), and 23 patients (23.7%) had FVC, TLC, and D(LCO) values < 80% of predicted values, respectively. The 6MWD at 12 months was 511.0 m (SD, 89.8 m), which was higher than at 3 months (mean difference, 47.0 m; 95% confidence interval [CI], 31.8 to 62.1 m; p < 0.01) but not different from 6 months (mean difference, 9.7 m; 95% CI, - 4.4 to 23.8 m; p = 0.18). The 6MWD was lower than that for normal control subjects of the same age groups, and there was impairment of HRQoL at 12 months. Patients who required ICU admission (n = 31) showed higher CXR scores (1.6 [SD, 3.1]; vs 0.4 [SD, 1.1]; p = 0.04) and lower percentage of predicted FVC, TLC, and Dlco than those who did not, but there were no differences in 6MWD and health status.
Conclusion: Significant impairment in Dlco was noted in 23.7% of survivors 1 year after illness onset. Exercise capacity and health status of SARS survivors were remarkably lower than those of a normal population.
Figures
References
-
- Peiris JS, Yuen KY, Osterhaus AD. The severe acute respiratory syndrome. N Engl J Med. 2003;349:2431–2441. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
