

Current concepts in periodontal bioengineering
- PMID: 16238610
- PMCID: PMC2581520
- DOI: 10.1111/j.1601-6343.2005.00352.x
Current concepts in periodontal bioengineering
Abstract
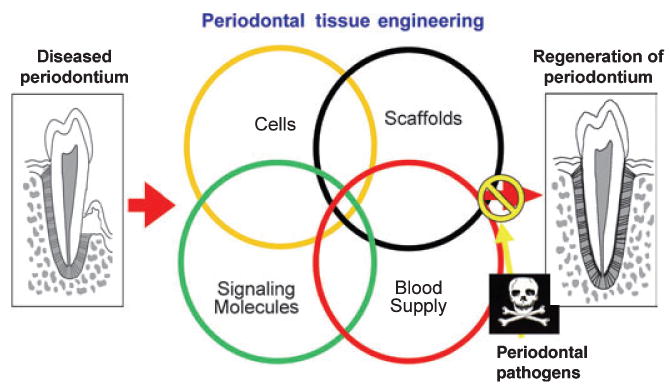
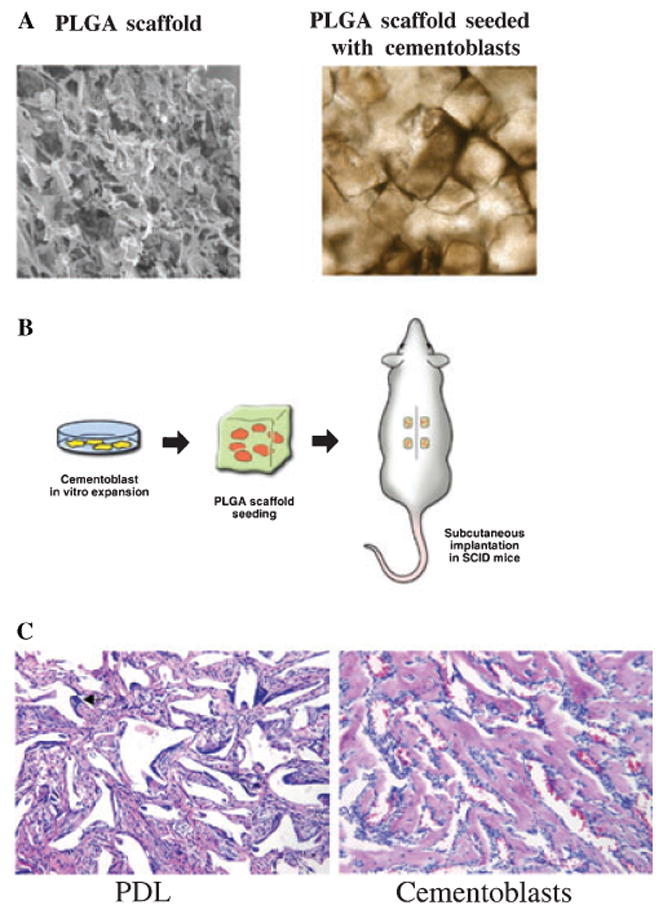
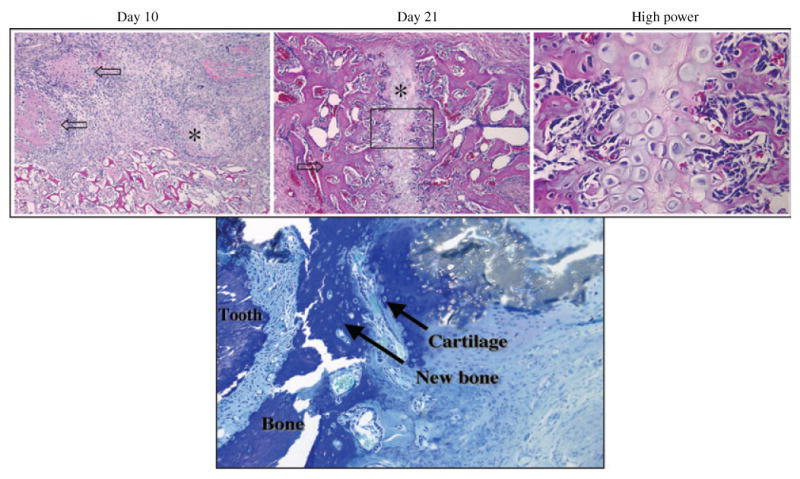
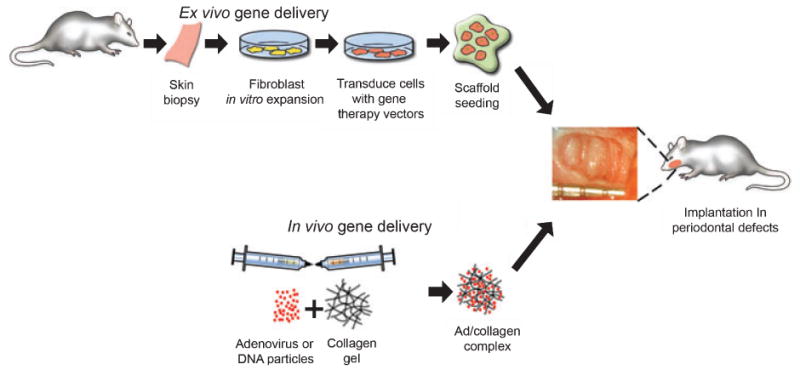
Repair of tooth supporting alveolar bone defects caused by periodontal and peri-implant tissue destruction is a major goal of reconstructive therapy. Oral and craniofacial tissue engineering has been achieved with limited success by the utilization of a variety of approaches such as cell-occlusive barrier membranes, bone substitutes and autogenous block grafting techniques. Signaling molecules such as growth factors have been used to restore lost tooth support because of damage by periodontal disease or trauma. This paper will review emerging periodontal therapies in the areas of materials science, growth factor biology and cell/gene therapy. Several different polymer delivery systems that aid in the targeting of proteins, genes and cells to periodontal and peri-implant defects will be highlighted. Results from preclinical and clinical trials will be reviewed using the topical application of bone morphogenetic proteins (BMP-2 and BMP-7) and platelet-derived growth factor-BB (PDGF) for periodontal and peri-implant regeneration. The paper concludes with recent research on the use of ex vivo and in vivo gene delivery strategies via gene therapy vectors encoding growth promoting and inhibiting molecules (PDGF, BMP, noggin and others) to regenerate periodontal structures including bone, periodontal ligament and cementum.
Figures
References
-
- Sipe JD, Kelley CA, McNichol LA. Reparative medicine: growing tissues and organs. Ann N Y Acad Sci. 2002;961:1–389. - PubMed
-
- Giannobile WV. Periodontal tissue engineering by growth factors. Bone. 1996;19(Suppl 1):23S–37S. - PubMed
-
- Albandar JM, Kingman A. Gingival recession, gingival bleeding, and dental calculus in adults 30 years of age and older in the United States, 1988–1994. J Periodontol. 1999;70:30–43. - PubMed
-
- Branemark PI. Rehabilitation and osseointegration in clinical reality. Int J Oral Maxillofac Implants. 2003;18:770–1. - PubMed
-
- Nakashima M, Reddi AH. The application of bone morphogenetic proteins to dental tissue engineering. Nat Biotechnol. 2003;21:1025–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
