

Visual evaluation of perfusion computed tomography in acute stroke accurately estimates infarct volume and tissue viability
- PMID: 16239323
- PMCID: PMC2077700
- DOI: 10.1136/jnnp.2005.074179
Visual evaluation of perfusion computed tomography in acute stroke accurately estimates infarct volume and tissue viability
Abstract
Objective: To establish the validity of visual interpretation of immediately processed perfusion computed tomography (CT) maps in acute stroke for prediction of final infarction.
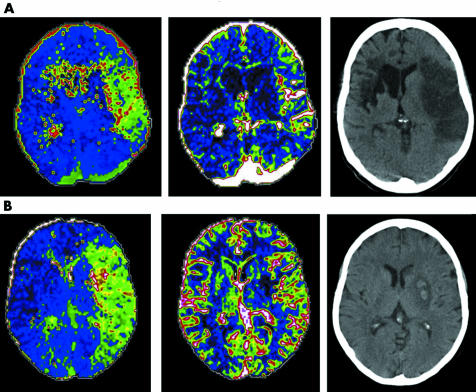
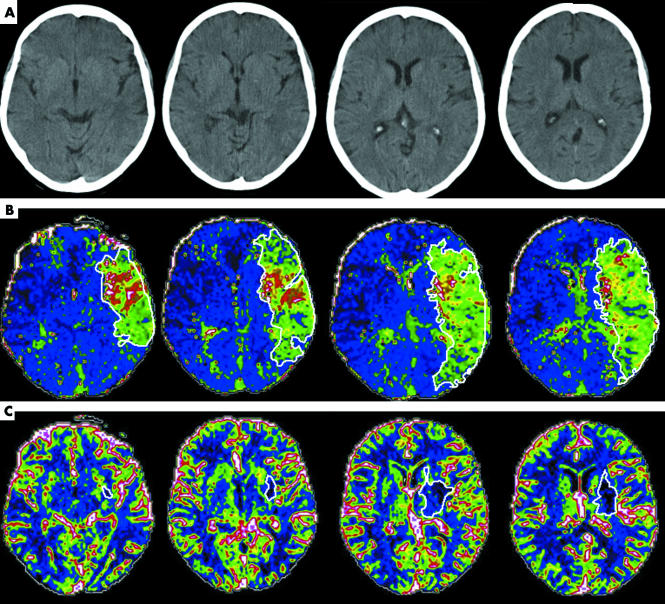
Methods: Perfusion CT studies acquired prospectively were reprocessed within six hours of stroke onset using standard CT console software. Four contiguous 5 mm thick images were obtained and maps of time to peak (TTP) and cerebral blood volume (CBV) generated. Volumes of lesions identified only by visual inspection were measured from manually drawn regions of interest. Volumes of tissue with prolonged TTP or reduced CBV were compared with independently calculated volume of infarction on non-contrast CT (NCCT) at 24-48 hours, and with clinical severity using the NIHSS score. Arterial patency at 24-48 h was included in analyses.
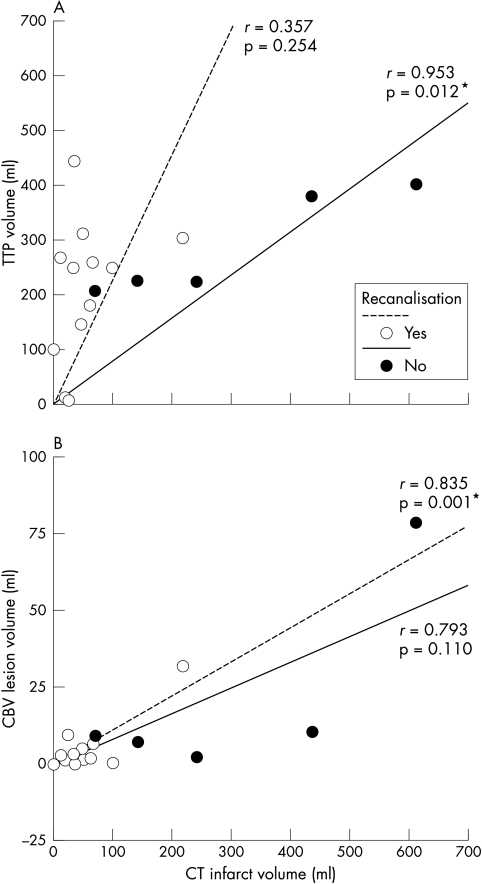
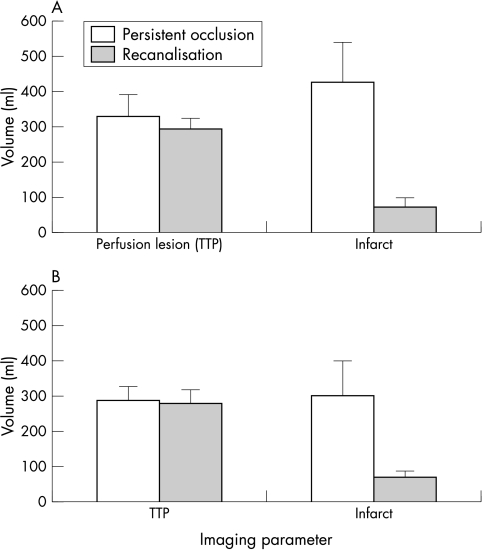
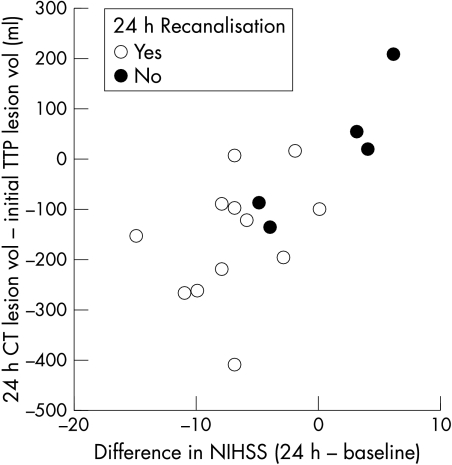
Results: Studies were analysed from 17 patients 150 minutes (median) after stroke onset. Volume of tissue with prolonged TTP correlated with initial NIHSS (r = 0.62, p = 0.009), and with NCCT final infarct volume when arterial occlusion persisted (r = 0.953, p = 0.012). Volume of tissue with reduced CBV correlated with final infarct volume if recanalisation occurred (r = 0.835, p = 0.001). Recanalisation was associated with lower 24 h NIHSS score (6 (IQR, 5 to 9.5) v 19 (18 to 26), p = 0.027), and in 10 patients given rtPA for MCA M1 occlusion, with lower infarct volume (73 v 431 ml, p = 0.002).
Conclusions: Visual evaluation of TTP and CBV maps generated by standard perfusion CT software correlated with 24-48 hour CT infarct volumes. Comparison of TTP and CBV maps yields information on tissue viability. Perfusion CT represents a practical technique to aid acute clinical decision making. Recanalisation was a crucial determinant of clinical and radiological outcome.
Conflict of interest statement
Competing interests: none declared
Similar articles
-
Multiphasic perfusion CT in acute middle cerebral artery ischemic stroke: prediction of final infarct volume and correlation with clinical outcome.Korean J Radiol. 2002 Jul-Sep;3(3):163-70. doi: 10.3348/kjr.2002.3.3.163. Korean J Radiol. 2002. PMID: 12271161 Free PMC article.
-
Comparison of perfusion computed tomography and computed tomography angiography source images with perfusion-weighted imaging and diffusion-weighted imaging in patients with acute stroke of less than 6 hours' duration.Stroke. 2004 Jul;35(7):1652-8. doi: 10.1161/01.STR.0000131271.54098.22. Epub 2004 May 20. Stroke. 2004. PMID: 15155964
-
Accuracy of the Alberta Stroke Program Early CT Score during the first 3 hours of middle cerebral artery stroke: comparison of noncontrast CT, CT angiography source images, and CT perfusion.AJNR Am J Neuroradiol. 2008 May;29(5):931-6. doi: 10.3174/ajnr.A0975. Epub 2008 Feb 13. AJNR Am J Neuroradiol. 2008. PMID: 18272553 Free PMC article.
-
Imaging viable brain tissue with CT scan during acute stroke.Cerebrovasc Dis. 2004;17 Suppl 3:28-34. doi: 10.1159/000075302. Cerebrovasc Dis. 2004. PMID: 14730256 Review.
-
Assessment of brain tissue viability under clinical circumstances.Acta Neurochir Suppl. 1999;73:73-80. doi: 10.1007/978-3-7091-6391-7_12. Acta Neurochir Suppl. 1999. PMID: 10494345 Review.
Cited by
-
Perfusion CT in acute stroke: prediction of vessel recanalization and clinical outcome in intravenous thrombolytic therapy.Eur Radiol. 2007 Oct;17(10):2491-8. doi: 10.1007/s00330-007-0696-9. Epub 2007 Jun 5. Eur Radiol. 2007. PMID: 17549483
-
Imaging-based treatment selection for intravenous and intra-arterial stroke therapies: a comprehensive review.Expert Rev Cardiovasc Ther. 2011 Jul;9(7):857-76. doi: 10.1586/erc.11.56. Expert Rev Cardiovasc Ther. 2011. PMID: 21809968 Free PMC article. Review.
-
Diffusion-perfusion mismatch: an opportunity for improvement in cortical function.Front Neurol. 2015 Jan 14;5:280. doi: 10.3389/fneur.2014.00280. eCollection 2014. Front Neurol. 2015. PMID: 25642208 Free PMC article.
-
Clinical review: Imaging in ischaemic stroke--implications for acute management.Crit Care. 2007;11(5):227. doi: 10.1186/cc5973. Crit Care. 2007. PMID: 17875224 Free PMC article. Review.
-
Neuroimaging as a Selection Tool and Endpoint in Clinical and Pre-clinical Trials.Transl Stroke Res. 2016 Oct;7(5):368-77. doi: 10.1007/s12975-016-0487-1. Epub 2016 Aug 20. Transl Stroke Res. 2016. PMID: 27543177 Free PMC article. Review.
References
-
- Astrup J, Siesjo B K, Symon L. Thresholds in cerebral ischemia – the ischemic penumbra. Stroke 198112723–725. - PubMed