

Cost effectiveness of inhaled steroid withdrawal in outpatients with chronic obstructive pulmonary disease
- PMID: 16244087
- PMCID: PMC2080701
- DOI: 10.1136/thx.2005.044578
Cost effectiveness of inhaled steroid withdrawal in outpatients with chronic obstructive pulmonary disease
Abstract
Background: The evidence for the effectiveness and safety of inhaled corticosteroids (ICS) in chronic obstructive pulmonary disease (COPD) is inconclusive. This study determined the cost effectiveness of withdrawing fluticasone propionate (FP) in outpatients with COPD.
Methods: The cost effectiveness analysis was based on a randomised, placebo controlled FP withdrawal study. After a 4 month run in period on FP, patients were randomly assigned to continue FP 500 microg twice daily or to receive placebo for 6 months. A decision analytical model evaluated the 6 month incremental cost effectiveness of the ICS versus ICS withdrawal strategy. One way sensitivity analyses and a Monte Carlo simulation were performed to evaluate the robustness of the findings.
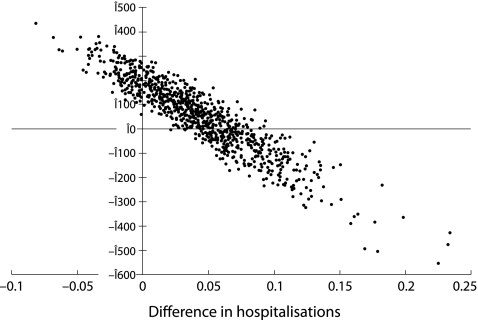
Results: The average patient with COPD in the FP group generated 511 in direct medical costs, including 238 for FP. The cost of the placebo strategy was 456. The higher direct drug cost of 212 per patient for the FP strategy during the 6 month follow up period compared with the placebo group was partially offset by a lower exacerbation and hospital admission cost of 157. The 6 month incremental cost effectiveness of the FP strategy compared with placebo was 110 per exacerbation prevented and 1286 per hospital admission prevented.
Conclusions: Over a 6 month period, withdrawing FP in a pre-selected trial population of COPD patients led to absolute cost savings but with a higher rate of exacerbations and hospital admissions.
Conflict of interest statement
Competing interests: none.



Similar articles
-
Withdrawal of fluticasone propionate from combined salmeterol/fluticasone treatment in patients with COPD causes immediate and sustained disease deterioration: a randomised controlled trial.Thorax. 2005 Jun;60(6):480-7. doi: 10.1136/thx.2004.034280. Thorax. 2005. PMID: 15923248 Free PMC article. Clinical Trial.
-
Cost effectiveness of therapy with combinations of long acting bronchodilators and inhaled steroids for treatment of COPD.Thorax. 2008 Nov;63(11):962-7. doi: 10.1136/thx.2007.089557. Epub 2008 Jul 11. Thorax. 2008. PMID: 18621985 Clinical Trial.
-
Effect of discontinuation of inhaled corticosteroids in patients with chronic obstructive pulmonary disease: the COPE study.Am J Respir Crit Care Med. 2002 Nov 15;166(10):1358-63. doi: 10.1164/rccm.200206-512OC. Epub 2002 Sep 5. Am J Respir Crit Care Med. 2002. PMID: 12406823 Clinical Trial.
-
[Introduction to asthma and chronic obstructive pulmonary disease pharmacoeconomics].Pol Merkur Lekarski. 2004 May;16 Suppl 1:5-6, 8. Pol Merkur Lekarski. 2004. PMID: 15524004 Review. Polish.
-
[Pharmaco-economics of asthma and chronic obstructive lung disease].Pol Merkur Lekarski. 2003 Jun;14(84):676-8. Pol Merkur Lekarski. 2003. PMID: 14524302 Review. Polish.
Cited by
-
Cost effectiveness of pharmacological maintenance treatment for chronic obstructive pulmonary disease: a review of the evidence and methodological issues.Pharmacoeconomics. 2012 Apr;30(4):271-302. doi: 10.2165/11589270-000000000-00000. Pharmacoeconomics. 2012. PMID: 22409290
-
New clinical insights into chronic obstructive pulmonary disease and their implications for pharmacoeconomic analyses.Pharmacoeconomics. 2012 Oct 1;30(10):869-85. doi: 10.2165/11633330-000000000-00000. Pharmacoeconomics. 2012. PMID: 22852587 Free PMC article. Review.
-
A new method for examining the cost savings of reducing COPD exacerbations.Pharmacoeconomics. 2010;28(9):733-49. doi: 10.2165/11535600-000000000-00000. Pharmacoeconomics. 2010. PMID: 20799755
References
-
- Lipworth B J. Systemic adverse effects of inhaled corticosteroid therapy: a systematic review and meta‐analysis. Arch Intern Med 1999159941–955. - PubMed
-
- Calverley P M. Inhaled corticosteroids are beneficial in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2000161341–342. - PubMed
-
- Barnes P J. Chronic obstructive pulmonary disease. N Engl J Med 2000343269–280. - PubMed
-
- Barnes P J. Inhaled corticosteroids are not beneficial in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2000161342–344. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical