

Mortality after acute myocardial infarction in hospitals that disproportionately treat black patients
- PMID: 16246963
- PMCID: PMC1626584
- DOI: 10.1161/CIRCULATIONAHA.105.543231
Mortality after acute myocardial infarction in hospitals that disproportionately treat black patients
Abstract
Background: African Americans are more likely to be seen by physicians with less clinical training or to be treated at hospitals with longer average times to acute reperfusion therapies. Less is known about differences in health outcomes. This report compares risk-adjusted mortality after acute myocardial infarction (AMI) between US hospitals with high and low fractions of elderly black AMI patients.
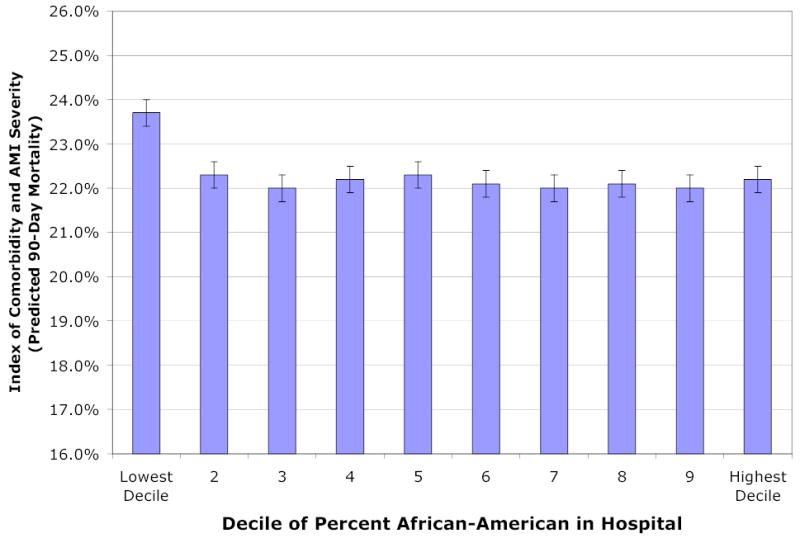
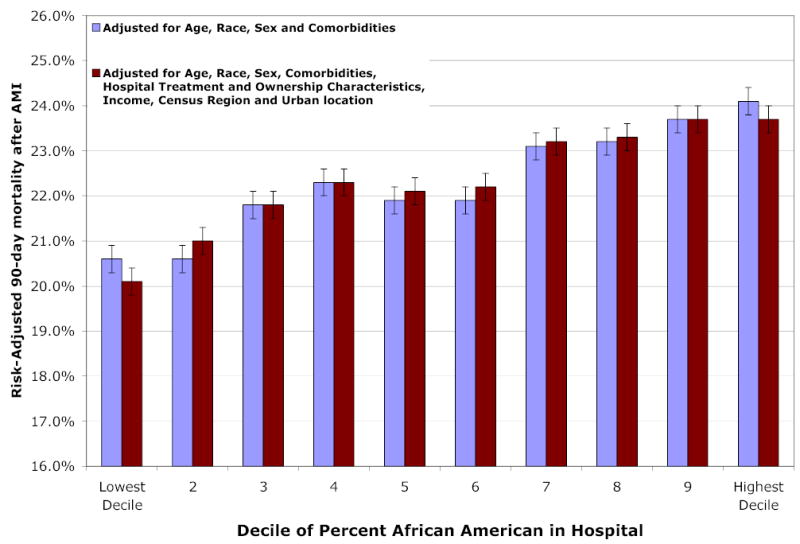
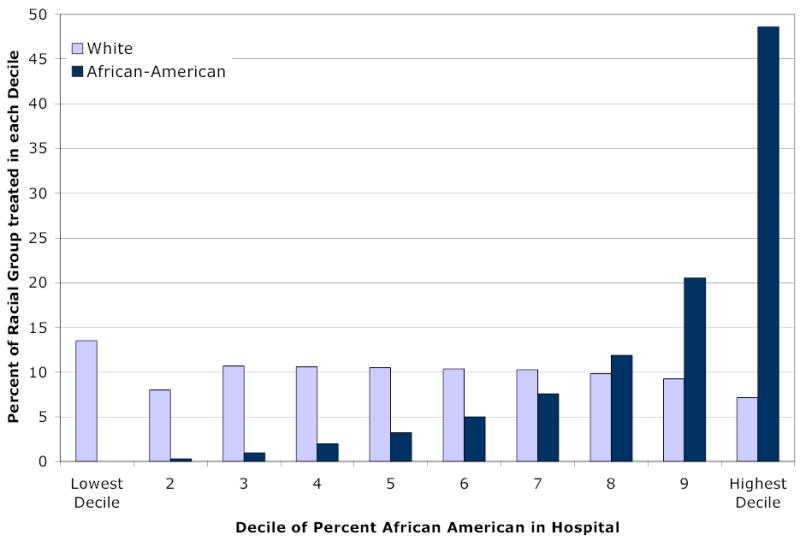
Methods and results: A prospective cohort study was performed for fee-for-service Medicare patients hospitalized for AMI during 1997 to 2001 (n=1,136,736). Hospitals (n=4289) were classified into approximate deciles depending on the extent to which the hospital served the black population. Decile 1 (12.5% of AMI patients) included hospitals without any black AMI admissions during 1997 to 2001. Decile 10 (10% of AMI patients) included hospitals with the highest fraction of black AMI patients (33.6%). The main outcome measures were 90-day and 30-day mortality after AMI. Patients admitted to hospitals disproportionately serving blacks experienced no greater level of morbidities or severity of the infarction, yet hospitals in decile 10 experienced a risk-adjusted 90-day mortality rate of 23.7% (95% CI 23.2% to 24.2%) compared with 20.1% (95% CI 19.7% to 20.4%) in decile 1 hospitals. Differences in outcomes between hospitals were not explained by income, hospital ownership status, hospital volume, census region, urban status, or hospital surgical treatment intensity.
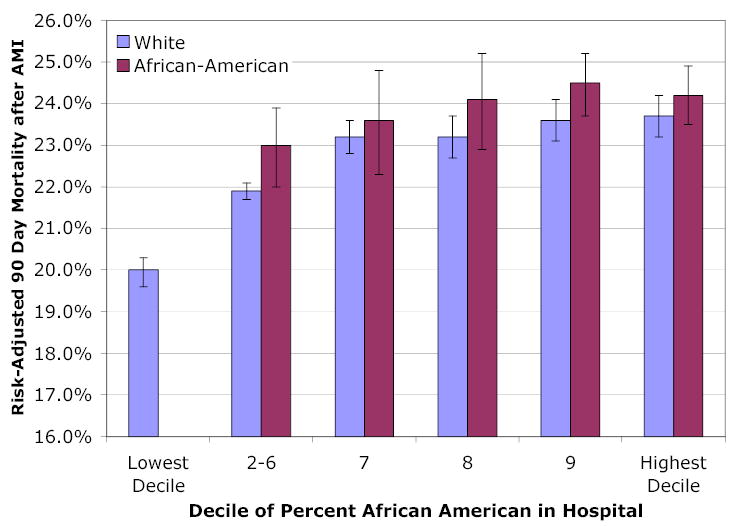
Conclusions: Risk-adjusted mortality after AMI is significantly higher in US hospitals that disproportionately serve blacks. A reduction in overall mortality at these hospitals could dramatically reduce black-white disparities in healthcare outcomes.
Conflict of interest statement
None.
Figures
Comment in
-
Separate but not equal: the consequences of segregated health care.Circulation. 2005 Oct 25;112(17):2582-4. doi: 10.1161/CIRCULATIONAHA.105.577635. Circulation. 2005. PMID: 16246956 Free PMC article. No abstract available.
References
-
- Smedley B, Stith A, Nelson A, editors. Unequal Treatment: Contronting Racial and Ethnic Disparities in Health Care. Washington DC: Institute of Medicine; 2002. - PubMed
-
- Borzak S, Joseph C, Havstad S, Tilley B, Smith ST, Housholder SD, Gheorghiade M. Lower thrombolytic use for African Americans with myocardial infarction: an influence of clinical presentation? American Heart Journal. 1999;137:338–45. - PubMed
-
- Ayanian J, Udvarhelyi I, Gatsonis C, Pashos C, Epstein A. Racial Differences in the Use of Revascularization Procedures After Coronary Angiography. Journal of the American Medical Association. 1993;269:2642–6. - PubMed
-
- Allison JJ, Kiefe CI, Centor RM, Box JB, Farmer RM. Racial differences in the medical treatment of elderly Medicare patients with acute myocardial infarction. Journal of General Internal Medicine. 1996;11:736–43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
