

Early and innovative interventions for severe sepsis and septic shock: taking advantage of a window of opportunity
- PMID: 16247103
- PMCID: PMC1266331
- DOI: 10.1503/cmaj.050632
Early and innovative interventions for severe sepsis and septic shock: taking advantage of a window of opportunity
Abstract
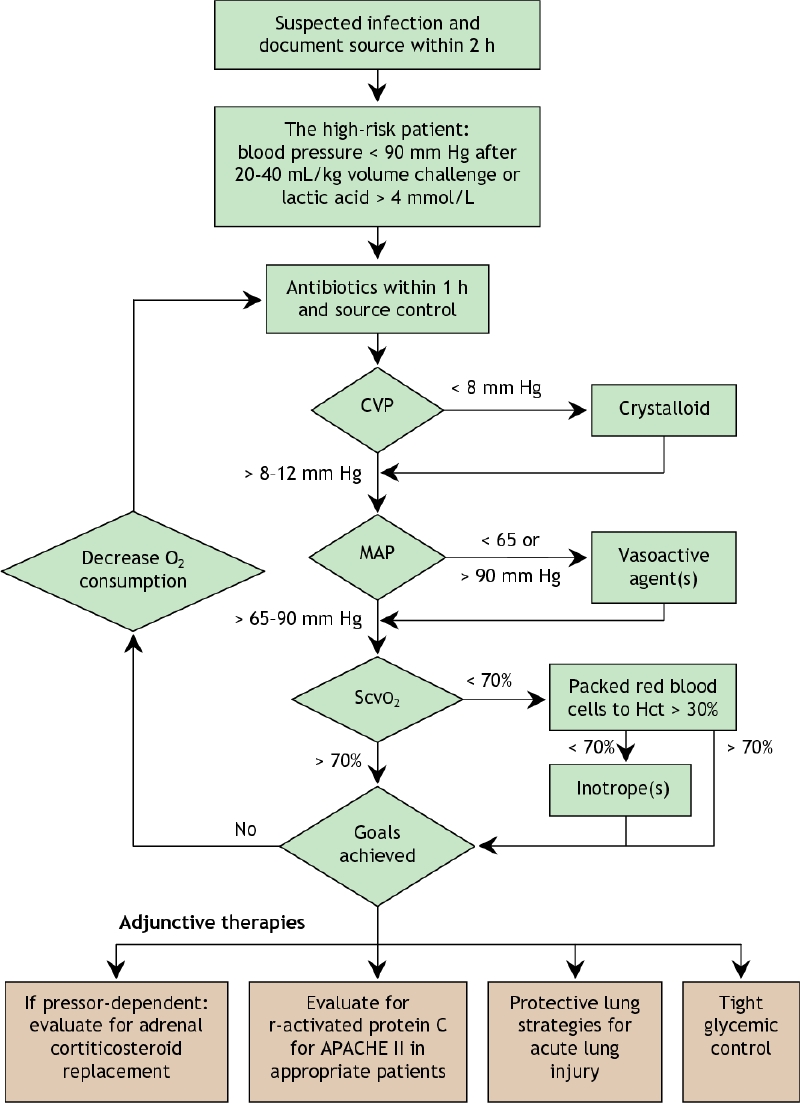
The pathogenic, diagnostic and therapeutic landscape of sepsis is no longer confined to the intensive care unit: many patients from other portals of entry to care, both outside and within the hospital, progress to severe disease. Approaches that have led to improved outcomes with other diseases (e.g., acute myocardial infarction, stroke and trauma) can now be similarly applied to sepsis. Improved understanding of the pathogenesis of severe sepsis and septic shock has led to the development of new therapies that place importance on early identification and aggressive management. This review emphasizes approaches to the early recognition, diagnosis and therapeutic management of sepsis, giving the clinician the most contemporary and practical approaches with which to treat these patients.
Figures

Similar articles
-
Outcome of patients with acute kidney injury in severe sepsis and septic shock treated with early goal-directed therapy in an intensive care unit.Saudi J Kidney Dis Transpl. 2014 May;25(3):544-51. doi: 10.4103/1319-2442.132171. Saudi J Kidney Dis Transpl. 2014. PMID: 24821150
-
Sepsis and septic shock.Emerg Med Clin North Am. 1986 Nov;4(4):809-40. Emerg Med Clin North Am. 1986. PMID: 3536440 Review.
-
Treatment of sepsis and septic shock: a review.Heart Lung. 1995 Sep-Oct;24(5):380-92; quiz 392-3. doi: 10.1016/s0147-9563(05)80059-7. Heart Lung. 1995. PMID: 8567303 Review.
-
Testing a conceptual model on early opening of the microcirculation in severe sepsis and septic shock: a randomised controlled pilot study.Eur J Anaesthesiol. 2015 Mar;32(3):189-98. doi: 10.1097/EJA.0000000000000126. Eur J Anaesthesiol. 2015. PMID: 25032942 Clinical Trial.
-
Stroke volume guided resuscitation in severe sepsis and septic shock improves outcomes.J Crit Care. 2017 Dec;42:42-46. doi: 10.1016/j.jcrc.2017.06.028. Epub 2017 Jun 28. J Crit Care. 2017. PMID: 28672146
Cited by
-
Human serum albumin improves arterial dysfunction during early resuscitation in mouse endotoxic model via reduced oxidative and nitrosative stresses.Am J Pathol. 2007 Dec;171(6):1753-61. doi: 10.2353/ajpath.2007.070316. Epub 2007 Nov 8. Am J Pathol. 2007. PMID: 17991713 Free PMC article.
-
Developing predictive models using electronic medical records: challenges and pitfalls.AMIA Annu Symp Proc. 2013 Nov 16;2013:1109-15. eCollection 2013. AMIA Annu Symp Proc. 2013. PMID: 24551396 Free PMC article.
-
The prevention of acute kidney injury: an in-depth narrative review Part 1: volume resuscitation and avoidance of drug- and nephrotoxin-induced AKI.NDT Plus. 2008 Dec;1(6):392-402. doi: 10.1093/ndtplus/sfn162. NDT Plus. 2008. PMID: 28657002 Free PMC article.
-
Identification of human pathogens isolated from blood using microarray hybridisation and signal pattern recognition.BMC Microbiol. 2007 Aug 14;7:78. doi: 10.1186/1471-2180-7-78. BMC Microbiol. 2007. PMID: 17697354 Free PMC article.
-
Skeletal muscle oxygen saturation does not estimate mixed venous oxygen saturation in patients with severe left heart failure and additional severe sepsis or septic shock.Crit Care. 2007;11(1):R6. doi: 10.1186/cc5153. Crit Care. 2007. PMID: 17227587 Free PMC article.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;29:1303-10. - PubMed
-
- Rivers EP, Nguyen HB, Huang DT, Donnino MW. Critical care and emergency medicine. Curr Opin Crit Care 2002;8:600-6. - PubMed
-
- McIntyre LA FD, Herbert PC, Cook DJ, Magder S, Dhingra V, Bell DR. Are delays in the recognition and initial management of patients with severe sepsis associated with hospital mortality? Crit Care Med 2003;31[12(Suppl)]:A75.
-
- Lundberg JS, Perl TM, Wiblin T, Costigan MD, Dawson J, Nettleman MD, et al. Septic shock: an analysis of outcomes for patients with onset on hospital wards versus intensive care units. Crit Care Med 1998;26:1020-4. - PubMed
-
- Lefrant JY, Muller L, Bruelle P, Pandolfi JL, L'Hermite J, Peray P, et al. Insertion time of the pulmonary artery catheter in critically ill patients. Crit Care Med 2000;28:355-9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical