Combining cytotoxic and immune-mediated gene therapy to treat brain tumors
- PMID: 16248789
- PMCID: PMC1629031
- DOI: 10.2174/156802605774370856
Combining cytotoxic and immune-mediated gene therapy to treat brain tumors
Abstract
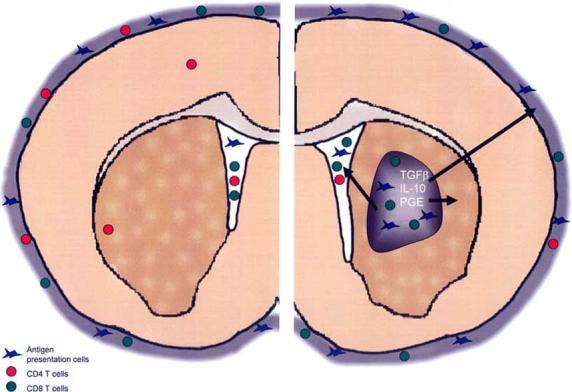
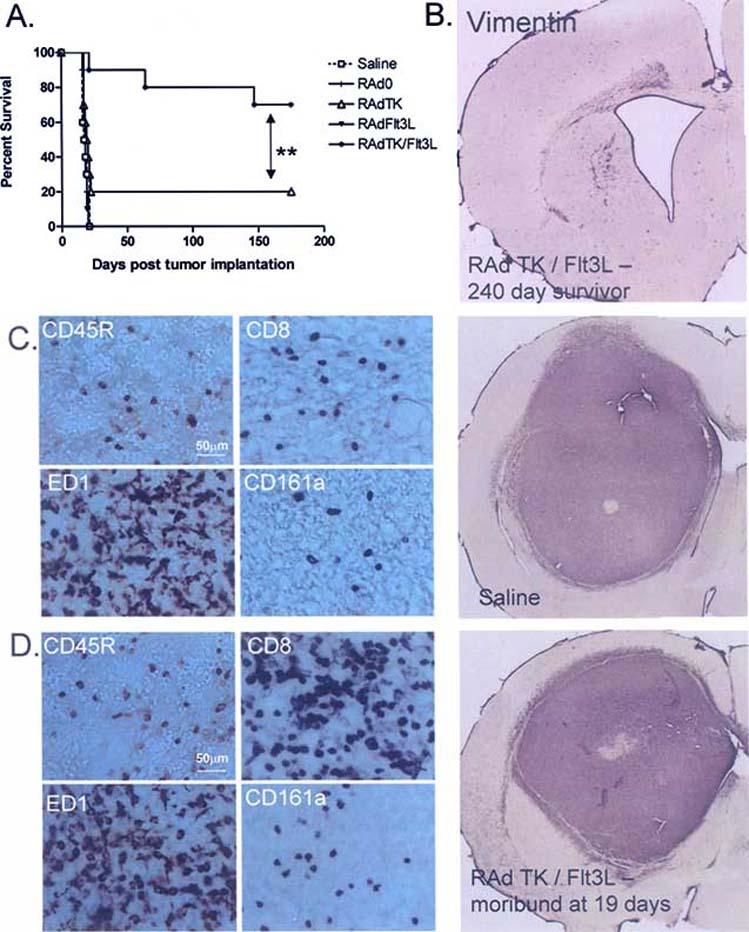
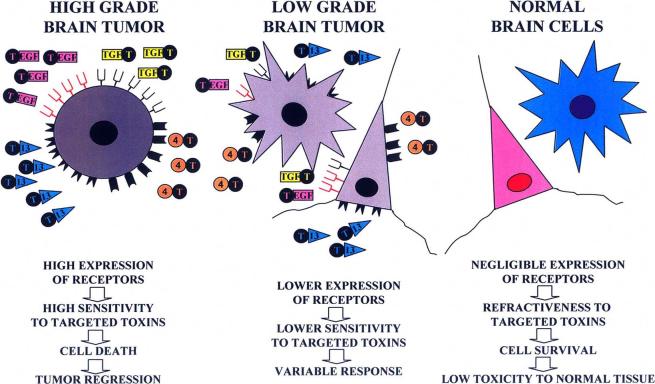
Glioblastoma (GBM) is a type of intracranial brain tumor, for which there is no cure. In spite of advances in surgery, chemotherapy and radiotherapy, patients die within a year of diagnosis. Therefore, there is a critical need to develop novel therapeutic approaches for this disease. Gene therapy, which is the use of genes or other nucleic acids as drugs, is a powerful new treatment strategy which can be developed to treat GBM. Several treatment modalities are amenable for gene therapy implementation, e.g. conditional cytotoxic approaches, targeted delivery of toxins into the tumor mass, immune stimulatory strategies, and these will all be the focus of this review. Both conditional cytotoxicity and targeted toxin mediated tumor death, are aimed at eliminating an established tumor mass and preventing further growth. Tumors employ several defensive strategies that suppress and inhibit anti-tumor immune responses. A better understanding of the mechanisms involved in eliciting anti-tumor immune responses has identified promising targets for immunotherapy. Immunotherapy is designed to aid the immune system to recognize and destroy tumor cells in order to eliminate the tumor burden. Also, immune-therapeutic strategies have the added advantage that an activated immune system has the capability of recognizing tumor cells at distant sites from the primary tumor, therefore targeting metastasis distant from the primary tumor locale. Pre-clinical models and clinical trials have demonstrated that in spite of their location within the central nervous system (CNS), a tissue described as 'immune privileged', brain tumors can be effectively targeted by the activated immune system following various immunotherapeutic strategies. This review will highlight recent advances in brain tumor immunotherapy, with particular emphasis on advances made using gene therapy strategies, as well as reviewing other novel therapies that can be used in combination with immunotherapy. Another important aspect of implementing gene therapy in the clinical arena is to be able to image the targeting of the therapeutics to the tumors, treatment effectiveness and progression of disease. We have therefore reviewed the most exciting non-invasive, in vivo imaging techniques which can be used in combination with gene therapy to monitor therapeutic efficacy over time.
Figures
References
-
- Ali-Osman F. Contemporary Cancer Research. Humana Press; Totowa: 2005. Brain Tumors.
-
- Legler JM, Ries LA, Smith MA, Warren JL, Heineman EF, Kaplan RS, Linet MS. Cancer surveillance series [corrected]: brain and other central nervous system cancers: recent trends in incidence and mortality. J. Natl. Cancer Inst. 1999;91(16):1382–90. - PubMed
-
- Surawicz TS, Davis F, Freels S, Laws ER, Jr., Menck HR. Brain tumor survival: results from the National Cancer Data Base. J. Neurooncol. 1998;40(2):151–60. - PubMed
-
- Platten M, Wick W, Weller M. Malignant glioma biology: role for TGF-beta in growth, motility, angiogenesis, and immune escape. Microsc. Res. Tech. 2001;52(4):401–10. - PubMed
-
- Yang L, Ng KY, Lillehei KO. Cell-mediated immunotherapy: a new approach to the treatment of malignant glioma. Cancer Control. 2003;10(2):138–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical