

Origin of interstitial fibroblasts in an accelerated model of angiotensin II-induced renal fibrosis
- PMID: 16251405
- PMCID: PMC1603794
- DOI: 10.1016/S0002-9440(10)61208-4
Origin of interstitial fibroblasts in an accelerated model of angiotensin II-induced renal fibrosis
Abstract
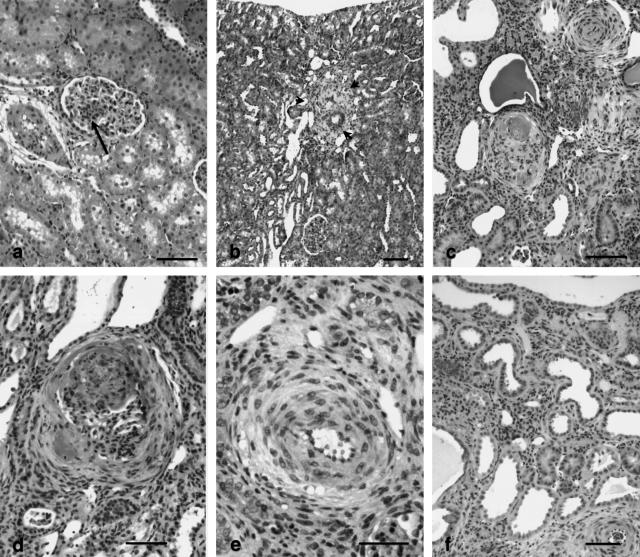
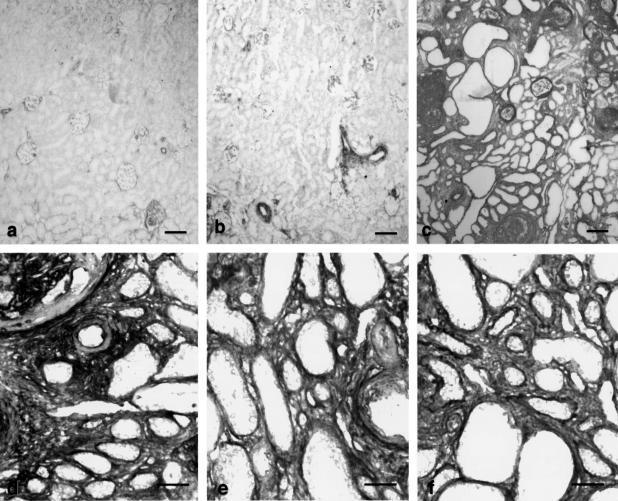
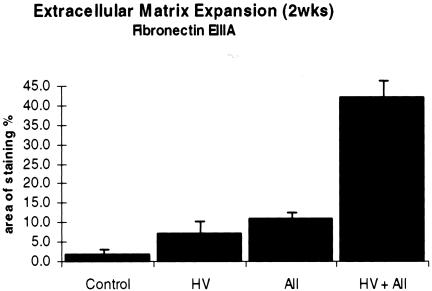
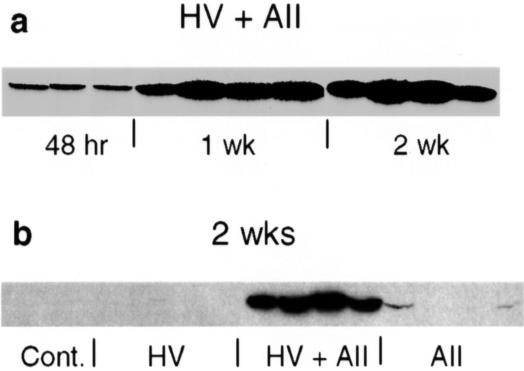
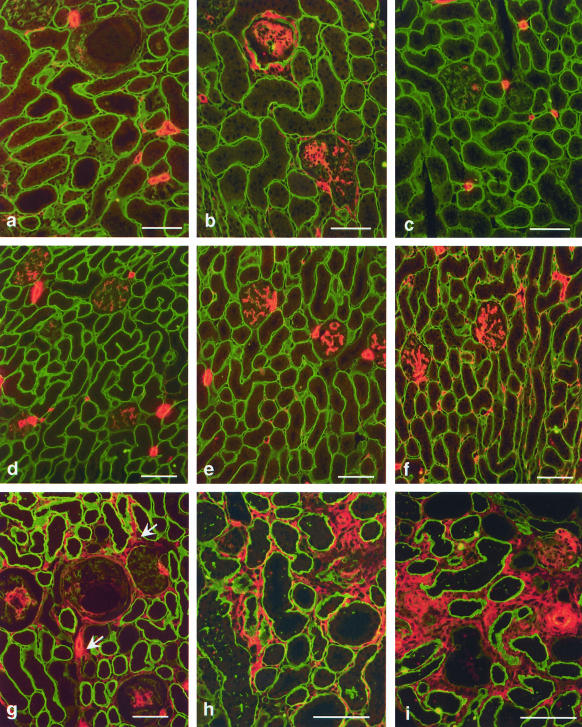
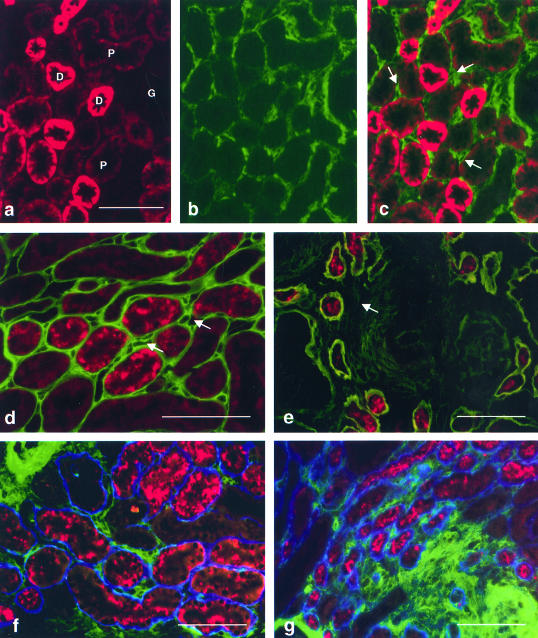
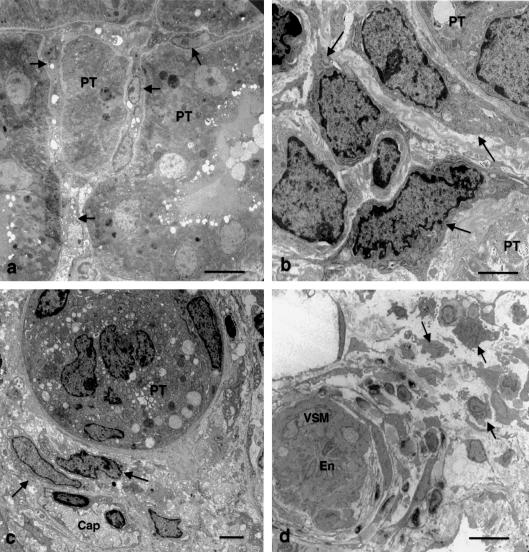
To determine whether previous renal injury accelerates the progression of glomerulosclerosis and interstitial fibrosis, we examined the effect of treating rats with angiotensin II after Habu venom injury. After initiating disease, we examined the origin of interstitial myofibroblasts by locating alpha-smooth muscle actin (alpha-SMA)-positive and Na+,K+-ATPase-positive cells relative to interstitial space, tubular epithelial cells, the tubular basement membrane (TBM), and vascular structures. Tubular epithelial-mesenchymal transition was also assessed by examining TBM integrity and by using Texas Red (TR)-dextran in intravital tracking experiments. The staining of alpha-SMA-positive myofibroblasts dramatically increased in peritubular interstitial spaces 48 hours after Habu venom plus angiotensin II, particularly in and around perivascular and periglomerular regions, while tubular epithelial cells were alpha-SMA-negative. Na+,K+-ATPase-positive and TR-dextran-labeled cells were restricted to the tubular epithelium and excluded from the interstitium. By 7 and 14 days, expanded interstitial space contained only alpha-SMA-positive myofibroblasts without TR-dextran endocytic particles. Epithelium of atrophic tubules containing TR-dextran remained confined by surrounding interstitium and myofibroblasts. These studies indicate that early expansion of alpha-SMA-positive cells in the interstitium and loss of tubular area occur via encroachment of interstitial myofibroblasts from perivascular into atrophic tubular spaces rather than via epithelial-mesenchymal transition and migration of tubular cells through the TBM into the interstitium.
Figures
References
-
- Border WA, Noble NA. Interactions of transforming growth factor-beta and angiotensin II in renal fibrosis. Hypertension. 1998;31:181–188. - PubMed
-
- Klahr S, Morrissey JJ. Comparative study of ACE inhibitors and angiotensin II receptor antagonists in interstitial scarring. Kidney Int. 1997;52:S111–S114. - PubMed
-
- Wolf G, Neilson EG. Angiotensin II as a renal growth factor. J Am Soc Nephrol. 1993;3:1531–1540. - PubMed
-
- Klahr S, Morrissey JJ. The role of vasoactive compounds, growth factors and cytokines in the progression of renal disease. Kidney Int. 2000;57:S7–S14. - PubMed
-
- Matsusaka T, Hymes J, Ichikawa I. Angiotensin in progressive renal diseases: theory and practice. J Am Soc Nephrol. 1996;7:2025–2043. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
