

Bacillus anthracis edema toxin causes extensive tissue lesions and rapid lethality in mice
- PMID: 16251415
- PMCID: PMC1603774
- DOI: 10.1016/S0002-9440(10)61218-7
Bacillus anthracis edema toxin causes extensive tissue lesions and rapid lethality in mice
Abstract
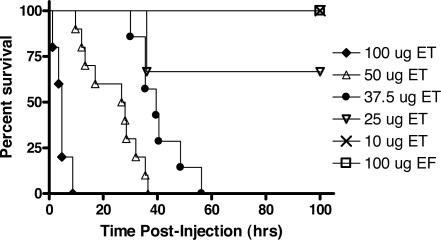
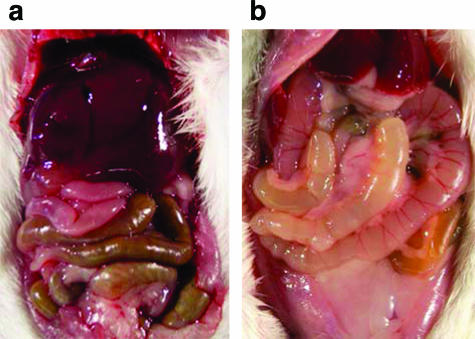
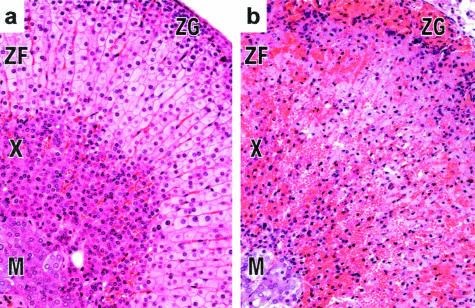
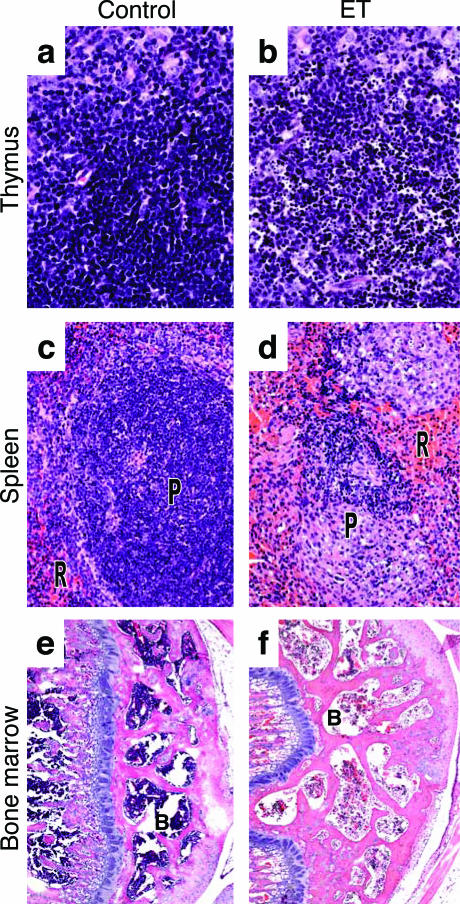
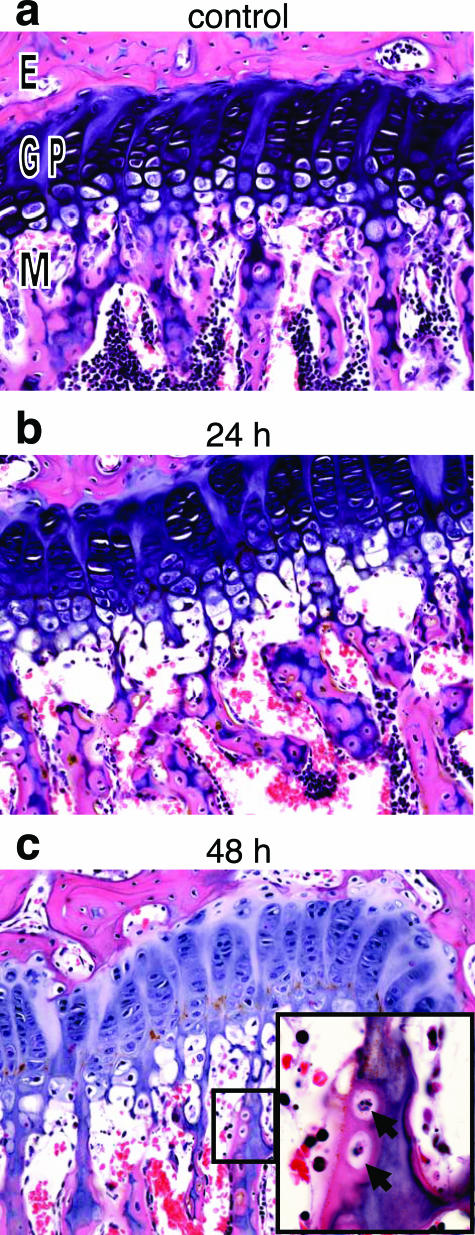
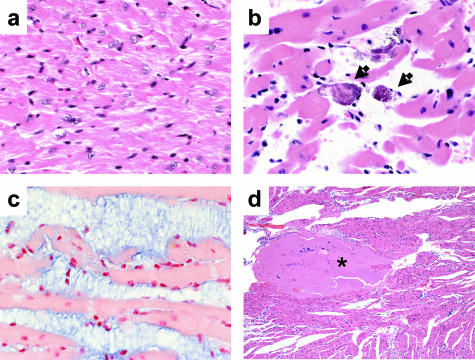
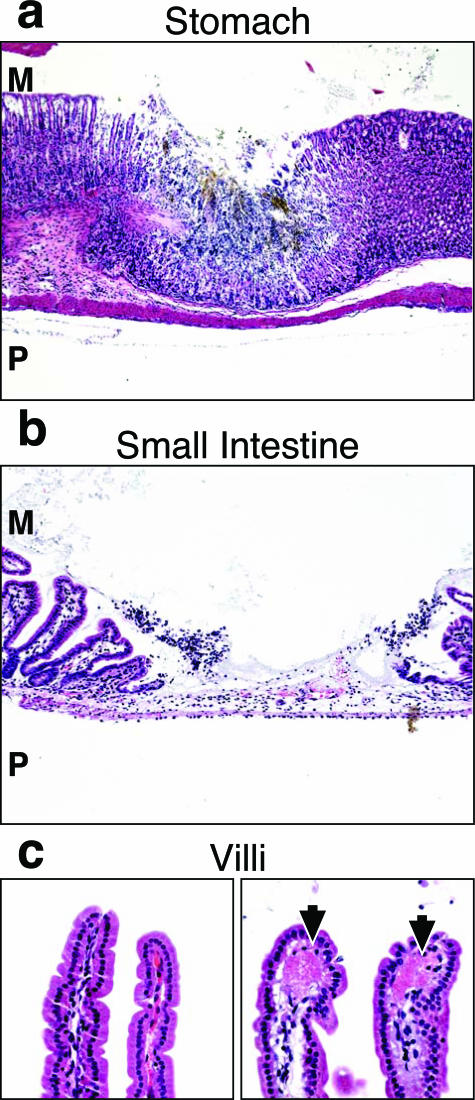
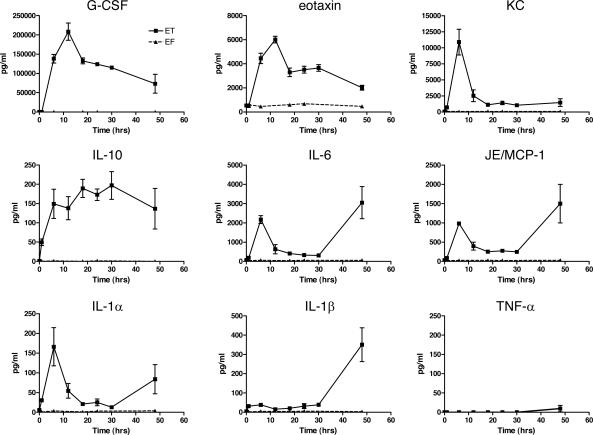
Bacillus anthracis edema toxin (ET), an adenylyl cyclase, is an important virulence factor that contributes to anthrax disease. The role of ET in anthrax pathogenesis is, however, poorly understood. Previous studies using crude toxin preparations associated ET with subcutaneous edema, and ET-deficient strains of B. anthracis showed a reduction in virulence. We report the first comprehensive study of ET-induced pathology in an animal model. Highly purified ET caused death in BALB/cJ mice at lower doses and more rapidly than previously seen with the other major B. anthracis virulence factor, lethal toxin. Observations of gross pathology showed intestinal intralumenal fluid accumulation followed by focal hemorrhaging of the ileum and adrenal glands. Histopathological analyses of timed tissue harvests revealed lesions in several tissues including adrenal glands, lymphoid organs, bone, bone marrow, gastrointestinal mucosa, heart, and kidneys. Concomitant blood chemistry analyses supported the induction of tissue damage. Several cytokines increased after ET administration, including granulocyte colony-stimulating factor, eotaxin, keratinocyte-derived cytokine, MCP-1/JE, interleukin-6, interleukin-10, and interleukin-1beta. Physiological measurements also revealed a concurrent hypotension and bradycardia. These studies detail the extensive pathological lesions caused by ET and suggest that it causes death due to multiorgan failure.
Figures

References
-
- Turnbull PC. Introduction: anthrax history, disease and ecology. Curr Top Microbiol Immunol. 2002;271:1–19. - PubMed
-
- Jernigan JA, Stephens DS, Ashford DA, Omenaca C, Topiel MS, Galbraith M, Tapper M, Fisk TL, Zaki S, Popovic T, Meyer RF, Quinn CP, Harper SA, Fridkin SK, Sejvar JJ, Shepard CW, McConnell M, Guarner J, Shieh WJ, Malecki JM, Gerberding JL, Hughes JM, Perkins BA. Bioterrorism-related inhalational anthrax: the first 10 cases reported in the United States. Emerg Infect Dis. 2001;7:933–944. - PMC - PubMed
-
- Kuehnert MJ, Doyle TJ, Hill HA, Bridges CB, Jernigan JA, Dull PM, Reissman DB, Ashford DA, Jernigan DB. Clinical features that discriminate inhalational anthrax from other acute respiratory illnesses. Clin Infect Dis. 2003;36:328–336. - PubMed
-
- Barakat LA, Quentzel HL, Jernigan JA, Kirschke DL, Griffith K, Spear SM, Kelley K, Barden D, Mayo D, Stephens DS, Popovic T, Marston C, Zaki SR, Guarner J, Shieh WJ, Carver HW, Meyer RF, Swerdlow DL, Mast EE, Hadler JL. Fatal inhalational anthrax in a 94-year-old Connecticut woman. JAMA. 2002;287:863–868. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
