

. 2005 Oct;18(4):311-9; discussion 319-20.
doi: 10.1080/08998280.2005.11928087.
New frontiers in radiosurgery for the brain and body
Affiliations
- PMID: 16252020
- PMCID: PMC1255939
- DOI: 10.1080/08998280.2005.11928087
Item in Clipboard
New frontiers in radiosurgery for the brain and body
Proc (Bayl Univ Med Cent).
2005 Oct.
Abstract
Radiosurgery is defined as the use of highly focused beams of radiation to ablate a pathologic target, thus achieving a surgical objective by noninvasive means. Recent advances have allowed a wide variety of intracranial lesions to be effectively treated with radiosurgery, and radiosurgical treatment has been accepted as a standard part of the neurosurgical armamentarium. The advent of frameless radiosurgery now permits radiosurgical treatment to all parts of the body and is being actively explored by many centers. This article reviews some of the modern tools for radiosurgical treatment and discusses the current clinical practice of radiosurgery.
Figures

Schematic showing the central idea of radiosurgery. The target (shown in red) receives a dose from each beam of radiation, whereas any other site receives a dose from only a single beam.

The Gamma Knife. The inset shows the collimator with 201 holes allowing 201 beams of radiation. During treatment, the Gamma Knife doors (arrow) open and the couch moves into the unit to position the head under the cobalt sources. Main photo courtesy of Elekta.
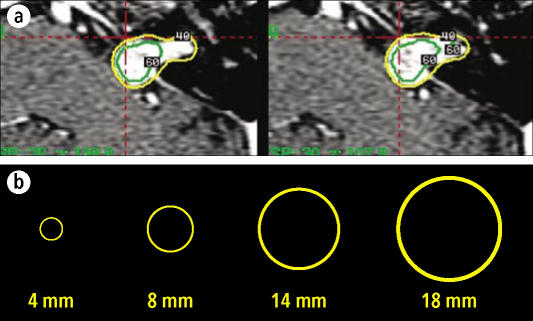
(a) Gamma Knife plans showing coverage of tumor with a 40% isodose line (shown in yellow) obtained by superimposing different spheres. (b) The Gamma Knife system includes collimators allowing creation of spheres of 4, 8, 14, and 18 mm.
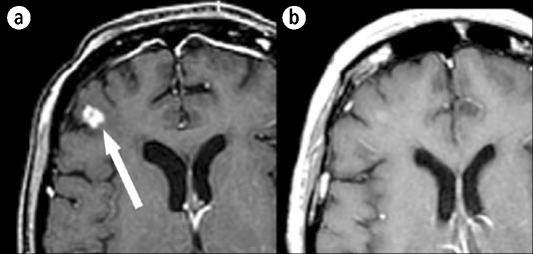
An MR image of a 57-year-old woman with non–small cell lung cancer, described in case example 1. (a) The right frontal lobe lesion at the time of Gamma Knife treatment. (b) The same region 3 months after treatment.

The CyberKnife. Arrow indicates the modified linear accelerator. Photo courtesy of Accuray.
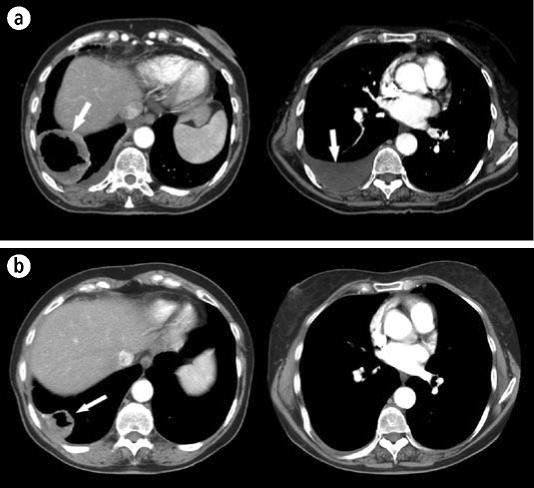
The patient described in case example 2. (a) A computed tomography scan of the chest at the time of CyberKnife treatment showing a large tumor (left) and pleural effusion (right). (b) The same regions 6 weeks after treatment. The tumor is significantly smaller, and pleural effusion has resolved. Arrows indicate tumor and effusion.
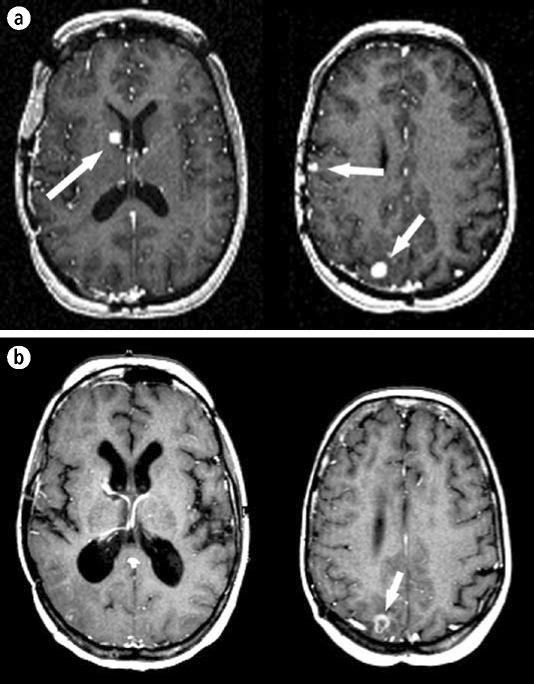
The patient described in case example 3. (a) An MR image of the head showing three lesions (arrows) due to metastatic ovarian cancer. (b) The same regions 6 years after treatment. Two of the lesions have resolved and one is smaller (arrow).
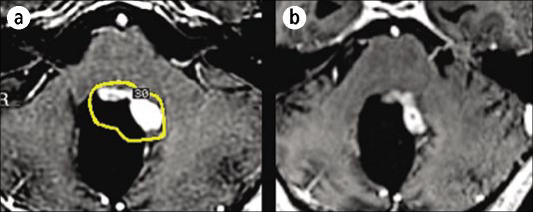
An MR scan of a 17-year-old male with a pilocytic astrocytoma treated with resection followed by external beam radiotherapy. (a) The tumor outlined by a 30% isodose line on the day of Gamma Knife treatment. (b) The same region 3 months later showing a significant decrease in tumor size. The dose was 13.5 Gy to the 30% isodose line.
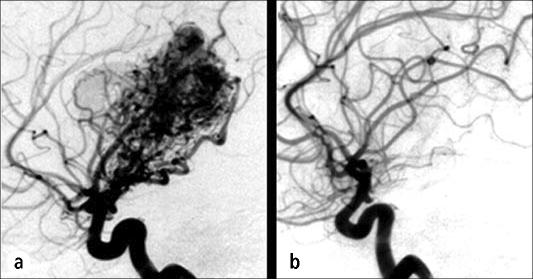
The patient described in case example 4. (a) An angiogram showing a thalamic arteriovenous malformation on the day of Gamma Knife treatment. (b) An angiogram 3 years after treatment showing resolution of the malformation.
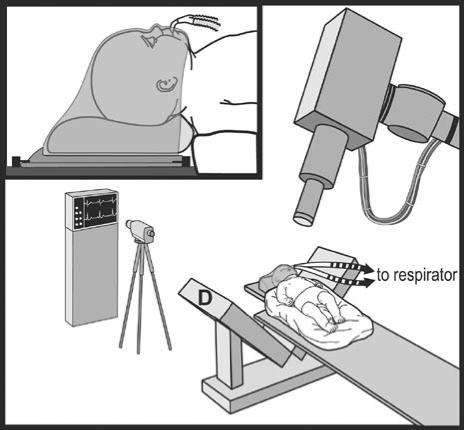
Schematic of the setup for CyberKnife treatment of infants. D indicates the x-ray detector of the CyberKnife system. Reprinted with permission from reference 48.
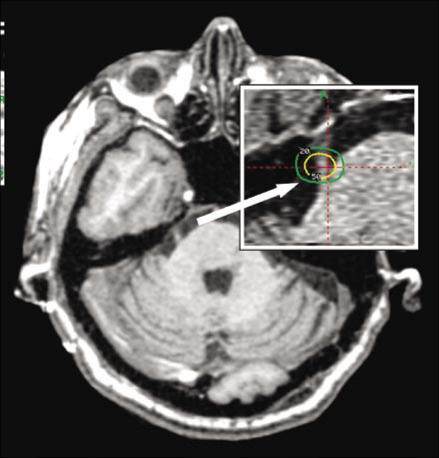
An MR image showing the trigeminal nerve. The inset shows targeting used in Gamma Knife radiosurgery for trigeminal neuralgia (the green line is the 20% isodose line and the yellow line is the 50% isodose line).
Similar articles
-
Regarding: Rosenthal DI, Glatstein E. "We've Got a Treatment, but What's the Disease?" The Oncologist 1996;1.Oncologist. 1997;2(1):59-61. Oncologist. 1997. PMID: 10388030
-
CyberKnife radiosurgery for brain metastases.Prog Neurol Surg. 2012;25:201-9. doi: 10.1159/000331193. Epub 2012 Jan 6. Prog Neurol Surg. 2012. PMID: 22236681 Review.
-
Current status and optimal use of radiosurgery.Oncology (Williston Park). 2001 Feb;15(2):209-16; discussion 219-21. Oncology (Williston Park). 2001. PMID: 11252934 Review.
-
Frame versus Frameless Leksell Stereotactic Radiosurgery.Prog Neurol Surg. 2019;34:19-27. doi: 10.1159/000493046. Epub 2019 May 16. Prog Neurol Surg. 2019. PMID: 31096212 Review.
-
CyberKnife frameless stereotactic radiosurgery for spinal lesions: clinical experience in 125 cases.Neurosurgery. 2004 Jul;55(1):89-98; discussion 98-9. Neurosurgery. 2004. PMID: 15214977 Clinical Trial.
Cited by
-
A lipoxygenase inhibitor in breast cancer brain metastases.J Neurooncol. 2007 Mar;82(1):91-3. doi: 10.1007/s11060-006-9248-4. Epub 2006 Sep 26. J Neurooncol. 2007. PMID: 17001517
-
Conventionally-fractionated image-guided intensity modulated radiotherapy (IG-IMRT): a safe and effective treatment for cancer spinal metastasis.Radiat Oncol. 2008 Apr 22;3:11. doi: 10.1186/1748-717X-3-11. Radiat Oncol. 2008. PMID: 18426607 Free PMC article.
-
Simulation of intrafraction motion and overall geometrical accuracy of a frameless intracranial radiosurgery process.J Appl Clin Med Phys. 2008 Oct 24;9(4):68-86. doi: 10.1120/jacmp.v9i4.2828. J Appl Clin Med Phys. 2008. PMID: 19020489 Free PMC article.
References
-
- Leksell L. Stereotaxis and Radiosurgery. Springfield, IL: Charles C. Thomas; 1971.
-
- Mack A, Czempiel H, Kreiner HJ, Durr G, Wowra B. Quality assurance in stereotactic space. A system test for verifying the accuracy of aim in radiosurgery. Med Phys. 2002;29:561–568. - PubMed
-
- Adler JR, Murphy MJ, Chang SD, Hancock SL. Image-guided robotic radiosurgery. Neurosurgery. 1999;44:1299–1307. - PubMed
-
- Kuo JS, Yu C, Petrovich Z, Apuzzo ML. The CyberKnife stereotactic radiosurgery system: description, installation, and an initial evaluation of use and functionality. Neurosurgery. 2003;53:1235–1239. - PubMed
-
- Chang SD, Main W, Martin DP, Gibbs IC, Heilbrun MP. An analysis of the accuracy of the CyberKnife: a robotic frameless stereotactic radiosurgical system. Neurosurgery. 2003;52:140–146. - PubMed
LinkOut - more resources
Full Text Sources