

doi: 10.1080/08998280.2005.11928089.
Use of PET/CT scanning in cancer patients: technical and practical considerations
Affiliations
- PMID: 16252023
- PMCID: PMC1255942
- DOI: 10.1080/08998280.2005.11928089
Item in Clipboard
Use of PET/CT scanning in cancer patients: technical and practical considerations
Proc (Bayl Univ Med Cent).
2005 Oct.
Abstract
This overview of the oncologic applications of positron emission tomography (PET) focuses on the technical aspects and clinical applications of a newer technique: the combination of a PET scanner and a computed tomography (CT) scanner in a single (PET/CT) device. Examples illustrate how PET/CT contributes to patient care and improves upon the previous state-of-the-art method of comparing a PET scan with a separate CT scan. Finally, the author presents some of the results from studies of PET/CT imaging that are beginning to appear in the literature.
Figures
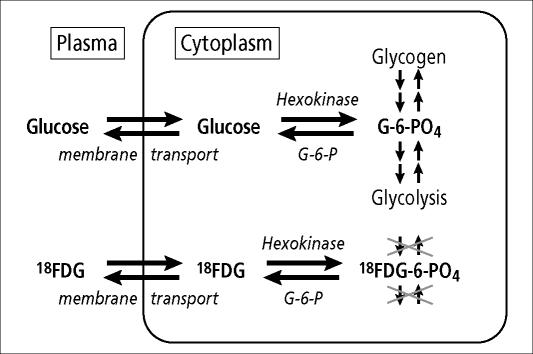
FDG is an analog of glucose in steps of membrane transport and phosphorylation but then becomes “metabolically trapped,” because it can be neither metabolized further nor stored as glycogen.
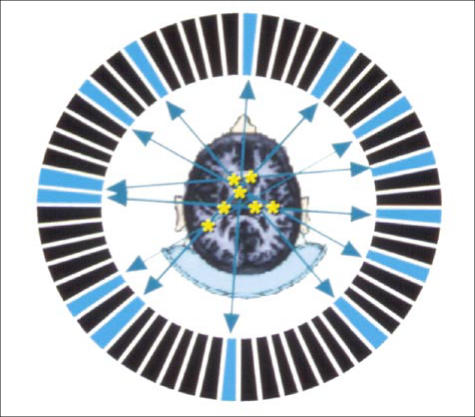
A ring of multiple specialized crystals detect the “coincidence” 511-keV photons resulting from positron decay and the subsequent annihilation reaction. Detection of enough coincident events allows reconstruction of an image of the distribution of tracer. This image depicts a transaxial slice through the brain, with the metabolically active gray matter showing much greater intensity than the less active white matter.

The General Electric Discovery ST PET/CT scanner in the North Texas Clinical PET Institute of the Baylor Sammons Cancer Center.

A patient with an infiltrative mass lesion in the left upper lobe, being evaluated for malignancy. (a) The CT scan shows a left upper lobe mass (arrow) and an enlarged mediastinal node (arrowhead). (b) The corresponding transaxial PET scan. (c) The fusion image shows intense hypermetabolism, suspicious for a malignant tumor (arrow) and metastatic node (arrowhead). Subsequent biopsy showed Mycobacterium avium-intracellulare infection.
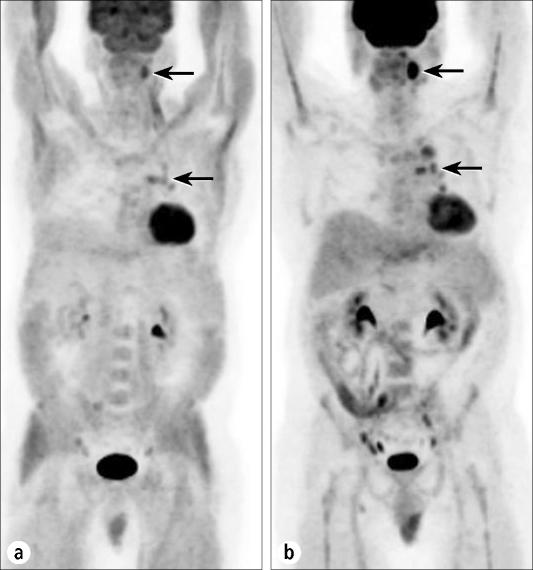
Anterior projection images from a PET scan of a patient undergoing staging of lymphoma. (a) The initial study was performed after the patient had eaten a candy bar 30 minutes prior to FDG injection. Note the extensive myocardial and muscle uptake due to high insulin levels. Diminished activity is seen in the brain and in tumor sites in the neck and chest (arrows). (b) A repeat study after the patient complied with routine fasting preparation shows more normal biodistribution of tracer and better visualization of tumor deposits (arrows).
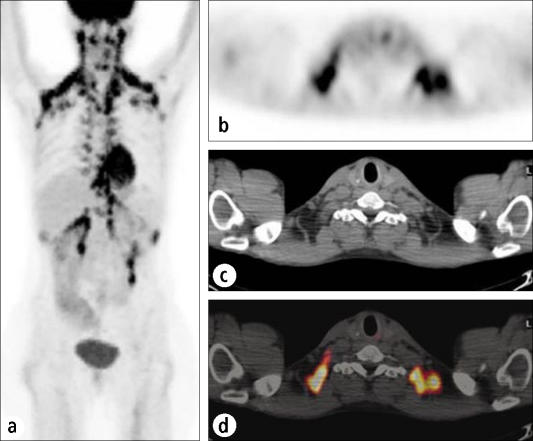
This case shows the effects of activation of brown fat in a nervous patient. (a) An anterior projection image shows abnormal activity extending from the neck through the supraclavicular and axillary regions, the anterior mediastinum, the paraspinal regions, and the retrocrural and perirenal regions. (b) Transaxial PET, (c) CT, and (d) fusion images localize the activity to fatty tissue rather than to lymph nodes or tumor masses.
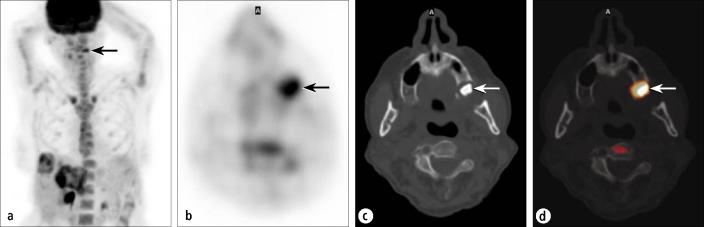
A patient being evaluated for metastatic colon cancer. (a) An anterior projection PET image shows known hepatic metastases, as well as an indeterminate focus in the left face (arrow). (b) Transaxial PET through the face shows a distinct hypermetabolic focus (arrow). The corresponding (c) CT and (d) fusion images show this focus to be a periodontal abscess in the maxillary alveolar ridge (arrows).

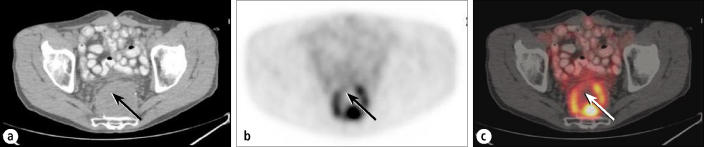
A patient being restaged for colon cancer. (a) PET image shows focal uptake consistent with recurrence (dashed circle) but does not allow localization. (b) CT and (c) fusion images show intraabdominal recurrence (arrow), as well as lesions involving the psoas and iliacus muscles (arrowheads). Lesser activity elsewhere is physiologic bowel uptake.
Recurrent rectal carcinoma. (a) A CT scan shows a large presacral mass that had yielded a negative biopsy result. The arrow shows the course of the needle biopsy. (b) PET and (c) fusion images show the discontinuous rim of the active tumor surrounding a necrotic center. Prior biopsy (arrrows show biopsy track) had passed through the zone of tumor into predominant necrosis. Repeat biopsy based on these images revealed tumor recurrence.
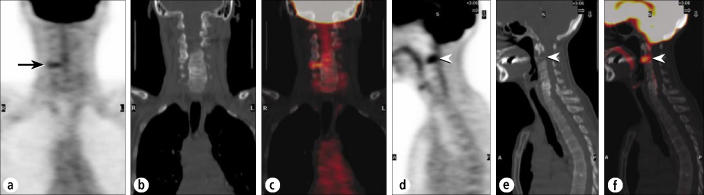
A patient being restaged for breast cancer. (a) A coronal PET image through the neck shows a small, linear focus in the lower right cervical spine (arrow). (b) Coronal CT and (c) fusion images show this to reflect facet arthropathy. (d) A sagittal PET image shows a more suspicious focus anteriorly (arrowhead), worrisome for metastasis (or possibly severe degenerative disk disease). (e) Sagittal CT and (f) fusion images show this to reflect a destructive metastasis in C2 (arrowheads).
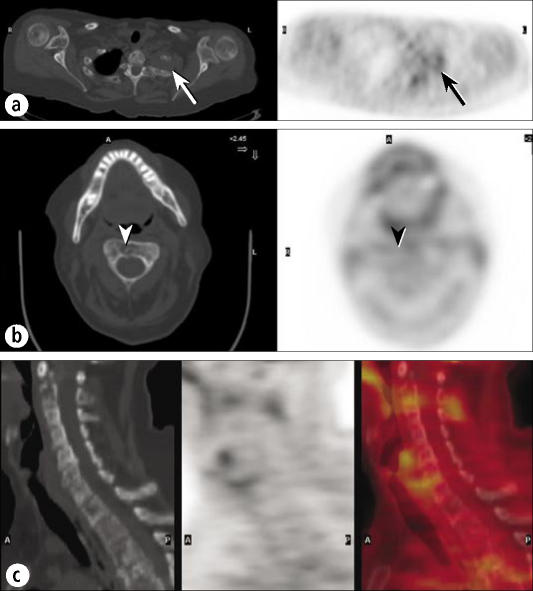
A patient with low-grade lymphoma. (a) PET and CT images through a left apical mass with rib involvement show only mild FDG uptake (arrows), very unusual for lymphoma. (b) A CT image through C2 clearly shows a destructive lesion (arrowhead), but a PET image shows minimal FDG uptake (arrowhead). (c) Sagittal CT, PET, and fusion images of the cervical spine show minimal or no FDG uptake in the extensive lytic disease seen on CT.
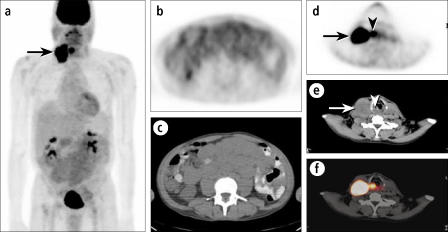
A patient with recurrent low-grade lymphoma of the abdomen and cervical adenopathy, presumed lymphomatous. (a) An anterior projection PET image shows intense uptake in the cervical adenopathy (arrow) but only mild FDG uptake in the diffuse abdominal involvement, seen better on transaxial images (b, c). The intense uptake seen in the cervical adenopathy (arrows) proved to be metastatic from a primary laryngeal carcinoma (arrowheads) (d, e, f).
Similar articles
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Positron emission tomography/computed tomography--imaging protocols, artifacts, and pitfalls.Mol Imaging Biol. 2004 Jul-Aug;6(4):188-99. doi: 10.1016/j.mibio.2004.04.006. Mol Imaging Biol. 2004. PMID: 15262234 Review.
-
Clinical practice guidelines for the utilization of positron emission tomography/computed tomography imaging in selected oncologic applications: suggestions from a provider group.Mol Imaging Biol. 2007 Nov-Dec;9(6):324-32; discussion 323. doi: 10.1007/s11307-007-0106-3. Mol Imaging Biol. 2007. PMID: 17701257
-
Comprehensive Oncologic Imaging in Infants and Preschool Children With Substantially Reduced Radiation Exposure Using Combined Simultaneous ¹⁸F-Fluorodeoxyglucose Positron Emission Tomography/Magnetic Resonance Imaging: A Direct Comparison to ¹⁸F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography.Invest Radiol. 2016 Jan;51(1):7-14. doi: 10.1097/RLI.0000000000000200. Invest Radiol. 2016. PMID: 26309185
-
Positron emission tomography/computed tomography.Semin Nucl Med. 2008 May;38(3):152-66. doi: 10.1053/j.semnuclmed.2008.01.003. Semin Nucl Med. 2008. PMID: 18396176 Review.
Cited by
-
Investigation of tumor assessment between two PET systems using various indices: comparison between PET/CT and PET/MRI systems.Am J Nucl Med Mol Imaging. 2023 Aug 15;13(4):156-163. eCollection 2023. Am J Nucl Med Mol Imaging. 2023. PMID: 37736495 Free PMC article.
-
Cancer and positron emission tomography imaging in India: Vision 2025.Indian J Nucl Med. 2016 Oct-Dec;31(4):251-254. doi: 10.4103/0972-3919.190804. Indian J Nucl Med. 2016. PMID: 27833308 Free PMC article. No abstract available.
-
False-Negative 18F-Fluorodeoxyglucose PET/CT in Malignant Pleural Mesothelioma.Cureus. 2021 Aug 17;13(8):e17263. doi: 10.7759/cureus.17263. eCollection 2021 Aug. Cureus. 2021. PMID: 34540486 Free PMC article.
-
Understanding Biologically Guided Radiotherapy: Essential Insights for Surgical Oncologists.Indian J Surg Oncol. 2024 Dec;15(Suppl 4):599-605. doi: 10.1007/s13193-024-02070-1. Epub 2024 Aug 21. Indian J Surg Oncol. 2024. PMID: 39995527 Review.
-
Stem Cells as a Novel Source for Regenerative Medicinal Applications in Alzheimer's Disease: An Update.Curr Mol Med. 2025;25(2):146-166. doi: 10.2174/0115665240334785240913071442. Curr Mol Med. 2025. PMID: 39318206 Review.
References
-
- Warburg O. In: The Metabolism of Tumors. Dickens F, editor. London: Constable; 1930. pp. 129–169.
-
- Beyer T, Townsend DW, Brun T, Kinahan PE, Charron M, Roddy R, Jerin J, Young J, Byars L, Nutt R. A combined PET/CT scanner for clinical oncology. J Nucl Med. 2000;41:1369–1379. - PubMed
-
- Lardinois D, Weder W, Hany TF, Kamel EM, Korom S, Seifert B, von Schulthess GK, Steinert HC. Staging of non–small-cell lung cancer with integrated positron-emission tomography and computed tomography. N Engl J Med. 2003;348:2500–2507. - PubMed
-
- Antoch G, Saoudi N, Kuehl H, Dahmen G, Mueller SP, Beyer T, Bockisch A, Debatin JF, Freudenberg LS. Accuracy of whole-body dual-modality fluorine-18–2-fluoro-2-deoxy-d-glucose positron emission tomography and computed tomography (FDG-PET/CT) for tumor staging in solid tumors: comparison with CT and PET. J Clin Oncol. 2004;22:4357–4368. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources