

Abdominal aortic aneurysm (AAA): cost-effectiveness of screening, surveillance of intermediate-sized AAA, and management of symptomatic AAA
- PMID: 16252027
- PMCID: PMC1255946
- DOI: 10.1080/08998280.2005.11928095
Abdominal aortic aneurysm (AAA): cost-effectiveness of screening, surveillance of intermediate-sized AAA, and management of symptomatic AAA
Abstract
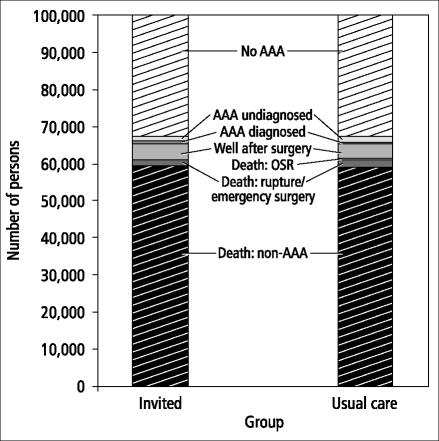
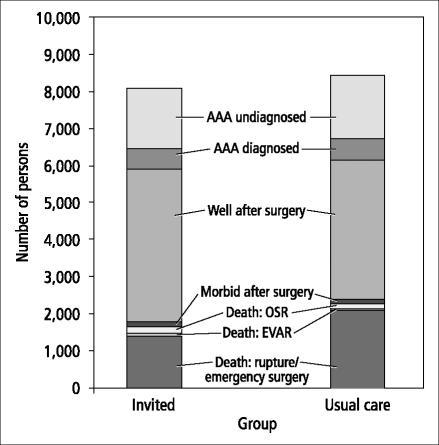
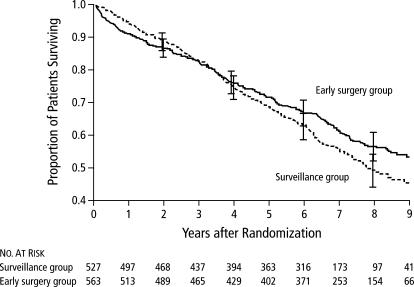
Physicians must make decisions about screening patients for abdominal aortic aneurysms (AAAs), monitoring or referring for surgery patients with AAAs of various sizes, and assessing patients with symptoms that may be related to AAAs. This review article analyzes the evidence for each scenario. The effectiveness and cost-effectiveness of screening for AAA is based on results from four randomized controlled trials. A cost-effectiveness analysis using a Markov model showed that ultrasound screening of white men beginning at age 65 is both effective and cost-effective in preventing AAA-related death. Such screening would have a small but real impact over a 20-year period in these men. For patients with a known AAA-which is often detected incidentally-the evidence clearly suggests periodic ultrasound surveillance for those with small AAAs (3.0-3.9 cm in diameter) and elective surgical repair for those with large AAAs (>or=5.5 cm). Two recent randomized controlled trials have shown that early surgical repair confers no survival benefit compared with periodic surveillance for patients with intermediate-sized AAAs (4.0-5.5 cm in diameter), so those patients can also be monitored. Some centers choose to increase the frequency of monitoring to every 3 to 6 months when the AAA reaches 5.0 cm. Factors to consider in assessing symptomatic patients include the high risk of life-threatening conditions, the potential increased risk of death or poor outcome with delay in diagnosis, the limitations of ultrasound in identifying whether symptoms are due to known or suspected AAA, and the timely availability of computed tomography or other imaging tests. If available, computed tomography is preferred in patients with recent or severe symptoms, since it is better at detecting retroperitoneal hemorrhage and other complications and in providing preoperative definition of the anatomy.
Figures

References
-
- Powell JT, Greenhalgh RM. Clinical practice. Small abdominal aortic aneurysms. N Engl J Med. 2003;348:1895–1901. - PubMed
-
- Scott RA, Bridgewater SG, Ashton HA. Randomized clinical trial of screening for abdominal aortic aneurysm in women. Br J Surg. 2002;89:283–285. - PubMed
-
- Grimshaw GM, Thompson JM. The abnormal aorta: a statistical definition and strategy for monitoring change. Eur J Vasc Endovasc Surg. 1995;10:95–100. - PubMed
-
- Wilmink AB, Pleumeekers HJ, Hoes AW, Hubbard CS, Grobbee DE, Quick CR. The infrarenal aortic diameter in relation to age: only part of the population in older age groups shows an increase. Eur J Vasc Endovasc Surg. 1998;16:431–437. - PubMed
-
- Wilmink AB, Hubbard CS, Day NE, Quick CR. The incidence of small abdominal aortic aneurysms and the change in normal infrarenal aortic diameter: implications for screening. Eur J Vasc Endovasc Surg. 2001;21:165–170. - PubMed
LinkOut - more resources
Full Text Sources