

Clinical presentation and prognostic factors of Streptococcus pneumoniae meningitis according to the focus of infection
- PMID: 16253143
- PMCID: PMC1295586
- DOI: 10.1186/1471-2334-5-93
Clinical presentation and prognostic factors of Streptococcus pneumoniae meningitis according to the focus of infection
Abstract
Background: We conducted a nationwide study in Denmark to identify clinical features and prognostic factors in patients with Streptococcus pneumoniae according to the focus of infection.
Methods: Based on a nationwide registration, clinical information's was prospectively collected from all reported cases of pneumococcal meningitis during a 2-year period (1999-2000). Clinical and laboratory findings at admission, clinical course and outcome of the disease including follow-up audiological examinations were collected retrospectively. The focus of infection was determined according to the clinical diagnosis made by the physicians and after review of the medical records.
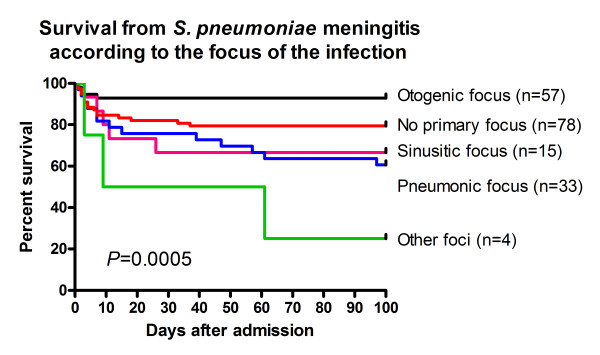
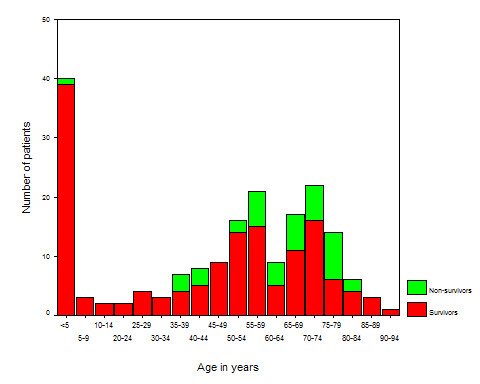
Results: 187 consecutive cases with S. pneumoniae meningitis were included in the study. The most common focus was ear (30%), followed by lung (18%), sinus (8%), and other (2%). In 42% of cases a primary infection focus could not be determined. On admission, fever and an altered mental status were the most frequent findings (in 93% and 94% of cases, respectively), whereas back rigidity, headache and convulsion were found in 57%, 41% and 11% of cases, respectively. 21% of patients died during hospitalisation (adults: 27% vs. children: 2%, Fisher Exact Test, P < 0.001), and the causes of death were due to neurological- and systemic complications or the combination of both in 8%, 5% and 6% of cases, respectively. Other causes (e.g. gastrointestinal bleeding, incurable cancer) accounted for 2% of cases. 41% of survivors had neurological sequelae (hearing loss: 24%, focal neurological deficits: 16%, and the combination of both: 1%). The mortality varied with the focus of the infection (otogenic: 7%, sinusitic: 33%, pneumonic: 26%, other kind of focus: 50%, no primary infection focus: 21%, Log rank test: P = 0.0005). Prognostic factors associated with fatal outcome in univariate logistic regression analysis were advanced age, presence of an underlying disease, history of headache, presence of a lung focus, absence of an otogenic focus, having a CT-scan prior to lumbar puncture, convulsions, requirement of assisted ventilation, and alterations in various CSF parameters (WBC < 500 cells/microL, high protein levels, glucose levels < 1 mmol/L, low CSF/blood glucose levels), P < 0.05. Independent prognostic factor associated with fatal outcome in multivariate logistic regression analysis was convulsions (OR: 4.53, 95%CI: (1.74-11.8), p = 0.002), whereas presence of an otogenic focus was independently associated with a better survival (OR: 6.09, 95%CI: (1.75-21.2), P = 0.005).
Conclusion: These results emphasize the prognostic importance of an early recognition of a predisposing focus to pneumococcal meningitis.
Figures
Similar articles
-
Mortality in pneumococcal meningitis: a multivariate analysis of prognostic factors.Eur J Med. 1993 Jan;2(1):28-32. Eur J Med. 1993. PMID: 8258002
-
Prehospital diagnostic and therapeutic management of otogenic Streptococcus pneumoniae meningitis.Scand J Infect Dis. 2006;38(3):172-80. doi: 10.1080/00365540500404060. Scand J Infect Dis. 2006. PMID: 16507498
-
Clinical features and prognostic factors in childhood pneumococcal meningitis.J Microbiol Immunol Infect. 2008 Feb;41(1):48-53. J Microbiol Immunol Infect. 2008. PMID: 18327426
-
Enterococcal meningitis: a clinical study of 39 cases and review of the literature.Medicine (Baltimore). 2003 Sep;82(5):346-64. doi: 10.1097/01.md.0000090402.56130.82. Medicine (Baltimore). 2003. PMID: 14530784 Review.
-
[Otogenic meningitis].Praxis (Bern 1994). 1998 Jun 10;87(24):839-44. Praxis (Bern 1994). 1998. PMID: 9658968 Review. German.
Cited by
-
Early symptomatic and late seizures in Kosovar children with bacterial meningitis.Childs Nerv Syst. 2011 Nov;27(11):1967-71. doi: 10.1007/s00381-011-1480-3. Epub 2011 May 20. Childs Nerv Syst. 2011. PMID: 21597996
-
Streptococcus pneumoniae Serotypes and Mortality in Adults and Adolescents in South Africa: Analysis of National Surveillance Data, 2003 - 2008.PLoS One. 2015 Oct 13;10(10):e0140185. doi: 10.1371/journal.pone.0140185. eCollection 2015. PLoS One. 2015. PMID: 26460800 Free PMC article.
-
Clinical Characteristics, Antimicrobial Resistance, and Outcomes of Patients with Invasive Pneumococcal Disease in Ningxia Hui Autonomous Region, China, 2013-2021.Can J Infect Dis Med Microbiol. 2022 Dec 12;2022:1262884. doi: 10.1155/2022/1262884. eCollection 2022. Can J Infect Dis Med Microbiol. 2022. PMID: 36545503 Free PMC article.
-
High cerebrospinal fluid (CSF) penetration and potent bactericidal activity in CSF of NZ2114, a novel plectasin variant, during experimental pneumococcal meningitis.Antimicrob Agents Chemother. 2009 Apr;53(4):1581-5. doi: 10.1128/AAC.01202-08. Epub 2009 Feb 2. Antimicrob Agents Chemother. 2009. PMID: 19188395 Free PMC article.
-
Clinical features, acute complications, and outcome of Salmonella meningitis in children under one year of age in Taiwan.BMC Infect Dis. 2011 Jan 27;11:30. doi: 10.1186/1471-2334-11-30. BMC Infect Dis. 2011. PMID: 21272341 Free PMC article.
References
-
- Auburtin M, Porcher R, Bruneel F, Scanvic A, Trouillet JL, Bedos JP, Regnier B, Wolff M. Pneumococcal meningitis in the intensive care unit: prognostic factors of clinical outcome in a series of 80 cases. Am J Respir Crit Care Med. 2002;165:713–717. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
