

Role of transmural dispersion of repolarization in the genesis of drug-induced torsades de pointes
- PMID: 16253930
- PMCID: PMC1479892
- DOI: 10.1016/j.hrthm.2004.09.011
Role of transmural dispersion of repolarization in the genesis of drug-induced torsades de pointes
Abstract
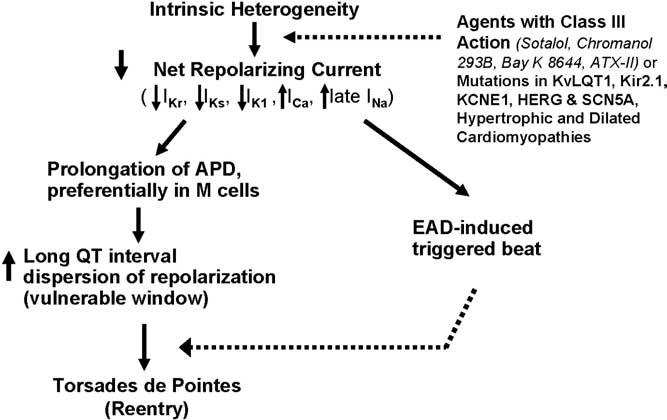
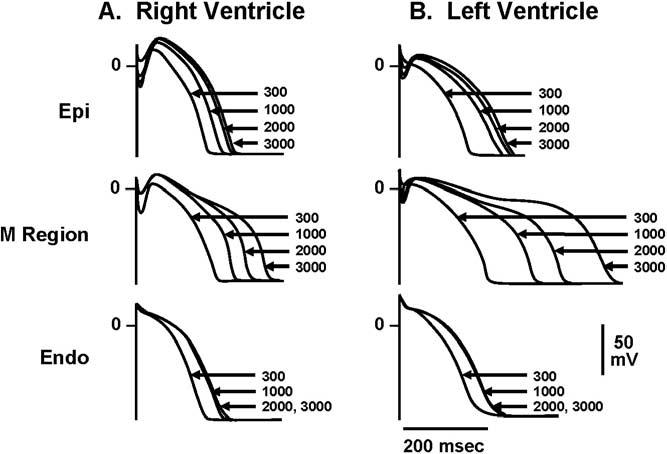
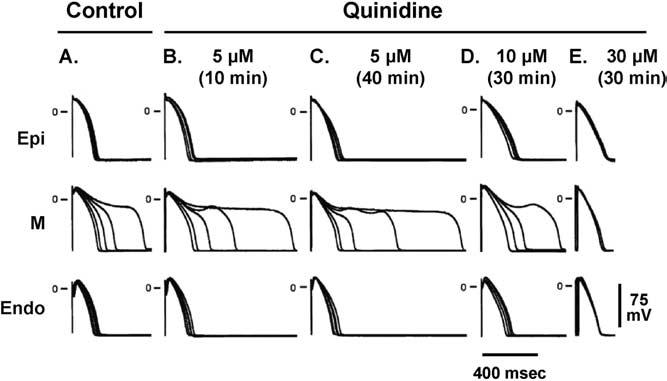
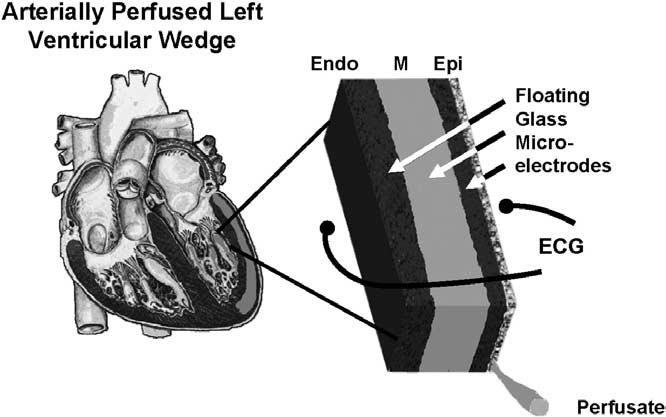
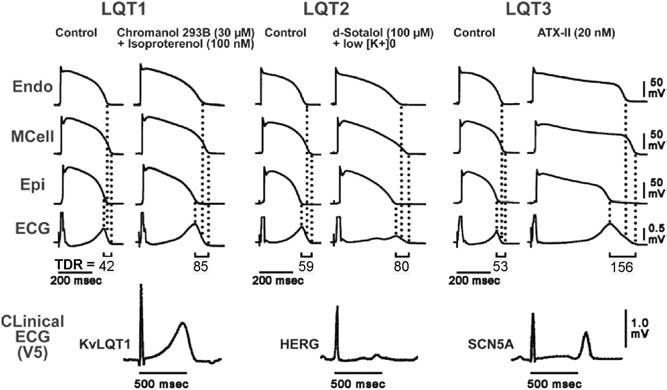
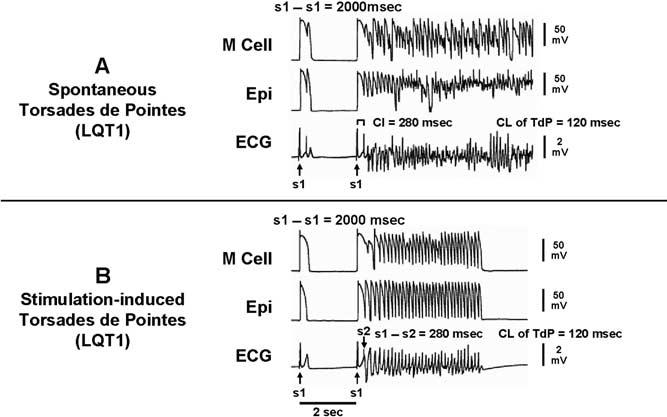
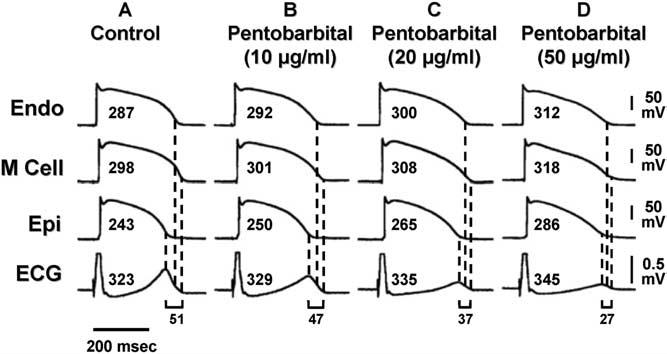
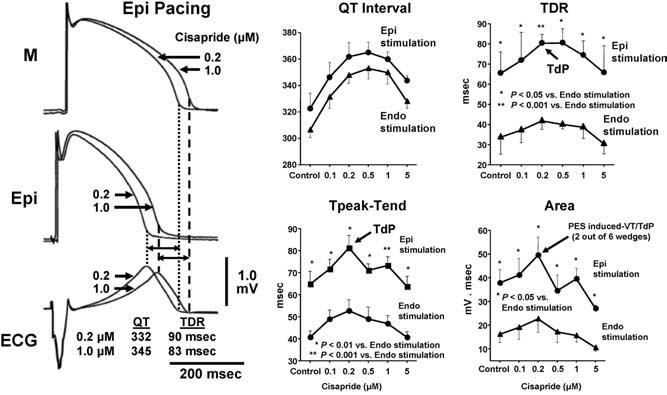
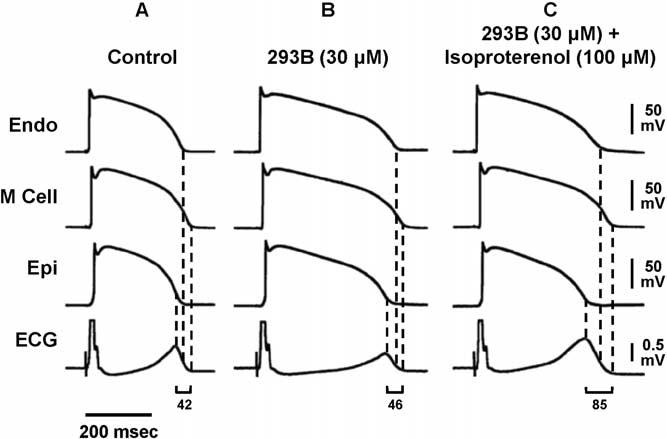
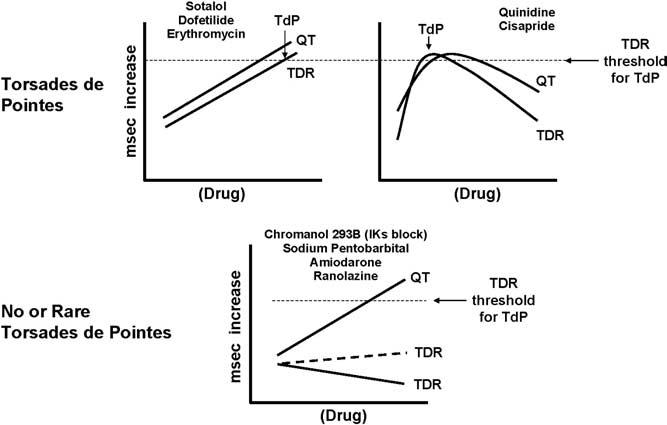
Torsades de pointes (TdP) is a potentially lethal arrhythmia that develops as a consequence of amplification of electrical heterogeneities intrinsic to the ventricular myocardium. These heterogeneities exist because of differences in the time course of repolarization of the three predominant cell types that make up the ventricular myocardium, giving rise to transmural voltage gradients and a dispersion of repolarization responsible for inscription of the ECG T wave. Antiarrhythmic agents with class III actions and/or the various mutations and cardiomyopathies associated with the long QT syndrome reduce net repolarizing current and amplify the intrinsic spatial dispersion of repolarization, thus creating the substrate for the development of reentry. The result is prolongation of the QT interval, abnormal T waves, and development of polymorphic reentrant ventricular tachycardia displaying characteristics of TdP. Prolongation of the QT interval apparently is not the sole determinant of a drug's potential to cause TdP. Agents that do not increase transmural dispersion of repolarization have little or no potential to induce TdP despite any ability to prolong the QT interval. In addition, drugs such as amiodarone and sodium pentobarbital can cause large QT prolongations but, by reducing transmural dispersion of repolarization, may reduce the likelihood of TdP. Arterially perfused wedge preparations of canine left ventricle can be used to explore the role of transmural dispersion of repolarization in the genesis of TdP. The purpose of this article is to review recent advances that have improved our understanding of these mechanisms, particularly the role of transmural dispersion of repolarization, in the genesis of drug-induced TdP and to examine how these advances can guide us toward the development of safer and more effective drugs.
Figures
References
-
- Keating M, Atkinson D, Dunn C, Timothy K, Vincent GM, Leppert M. Linkage of a cardiac arrhythmia, the long-QT syndrome, and the Harvey ras-1 gene. Science. 1991;252:704–706. - PubMed
-
- Antzelevitch C, Shimizu W. Cellular mechanisms underlying the long QT syndrome. Curr Opin Cardiol. 2002;17:43–51. - PubMed
-
- Antzelevitch C, Sicouri S, Litovsky SH, Lukas A, Krishnan SC, Di Diego JM, Gintant GA, Liu DW. Heterogeneity within the ventricular wall. Electrophysiology and pharmacology of epicardial, endocardial, and M cells. Circ Res. 1991;69:1427–1449. - PubMed
-
- Antzelevitch C, Shimizu W, Yan GX, Sicouri S, Weissenburger J, Nesterenko VV, Burashnikov A, Di Diego J, Saffitz J, Thomas GP. The M cell: its contribution to the ECG and to normal and abnormal electrical function of the heart. J Cardiovasc Electrophysiol. 1999;10:1124–1152. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
