

Anomaly of the left anterior descending coronary artery arising from the right sinus of valsalva and ventricular septal defect in adult: a rare case
- PMID: 16259076
- PMCID: PMC2810584
- DOI: 10.3349/ymj.2005.46.5.729
Anomaly of the left anterior descending coronary artery arising from the right sinus of valsalva and ventricular septal defect in adult: a rare case
Abstract
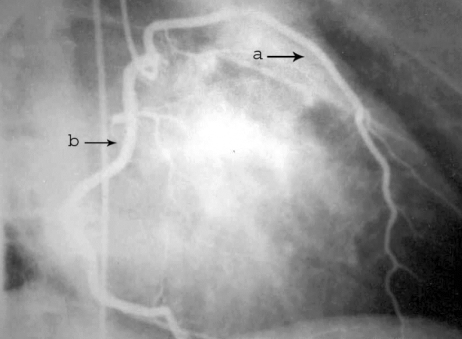
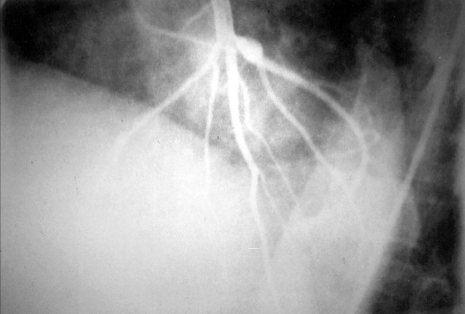
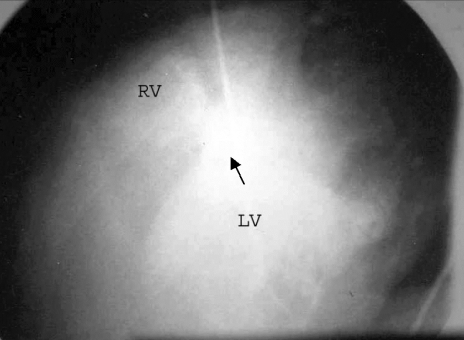
Anomaly of the left anterior descending (LAD) coronary artery arising from the right sinus of valsalva is frequently seen with tetralogy of Fallot (TOF). The association of the LAD coronary artery with ventricular septal defect (VSD) is uncommon. We described an anomalous origin of the LAD coronary artery from the right sinus of valsalva with ventricular septal defect in a 38-year-old male patient suffering from atypical angina. The LAD coronary artery arose from the right sinus of valsalva, just next to the right coronary artery. There was a single opening in the membranous part of the interventricular septum. From this case, we suggest that angiography is useful for both documenting anomalies of the LAD coronary artery associated with VSD and for determining the safest surgical procedures.
Figures
Similar articles
-
Anomalous origin of the left anterior descending coronary artery from the right sinus of Valsalva associated with effort angina pectoris.Eur Heart J. 1993 Jan;14(1):129-31. doi: 10.1093/eurheartj/14.1.129. Eur Heart J. 1993. PMID: 8432280
-
Anomalous left anterior descending coronary artery from pulmonary artery with ventricular septal defect.Ann Thorac Surg. 2007 Mar;83(3):1175-7. doi: 10.1016/j.athoracsur.2006.09.045. Ann Thorac Surg. 2007. PMID: 17307487
-
Clinical application of 64-slice spiral CT in the diagnosis of the Tetralogy of Fallot.Eur J Radiol. 2007 Nov;64(2):296-301. doi: 10.1016/j.ejrad.2007.02.026. Epub 2007 Mar 30. Eur J Radiol. 2007. PMID: 17399932
-
[Anomalous origin of the coronary arteries: five case reports and review of the literature].G Ital Cardiol (Rome). 2010 Oct;11(10):778-82. G Ital Cardiol (Rome). 2010. PMID: 21246781 Review. Italian.
-
Anomalous left coronary artery arising from right sinus of valsalva could be a minor congenital anomaly--a case report and review of the literature.Angiology. 1999 Feb;50(2):175-8. doi: 10.1177/000331979905000214. Angiology. 1999. PMID: 10063951 Review.
Cited by
-
A Case of Anomalous Left Anterior Descending Artery Originating From the Right Sinus of Valsalva.Cureus. 2021 Jun 10;13(6):e15584. doi: 10.7759/cureus.15584. eCollection 2021 Jun. Cureus. 2021. PMID: 34277205 Free PMC article.
-
A Rare Case of Multiple Anomalies of the Coronary Arteries.Cureus. 2018 Jun 13;10(6):e2796. doi: 10.7759/cureus.2796. Cureus. 2018. PMID: 30116675 Free PMC article.
-
A rare combination: Single coronary artery originating from the left sinus of valsalva coexisting with perimembranous ventricular septal defect.J Cardiol Cases. 2012 May 2;6(2):e39-e41. doi: 10.1016/j.jccase.2012.04.004. eCollection 2012 Aug. J Cardiol Cases. 2012. PMID: 30533067 Free PMC article.
References
-
- Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002;105:2449–2454. - PubMed
-
- McConnell MV, Ganz P, Selwyn AP, Li W, Edelman RR, Manning WJ. Identification of anomalous coronary arteries and their anatomic course by magnetic resonance coronary angiography. Circulation. 1995;92:3158–3162. - PubMed
-
- Martin GR, Perry LW, Ferencz C. Increased prevalence of ventricular septal defect: epidemic or improved diagnosis. Pediatrics. 1989;83:200–203. - PubMed
-
- Eugene B. Heart disease: A textbook of cardiovascular medicine. Second edition. Philadelphia, London, Toronto: W.B. Saunders Company; 1984. pp. 963–965.
-
- Hurts JW. The heart. 5th ed. New York: Mcgraw-Hill book company; 1982. pp. 672–680.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
