

Comparison of the systemic inflammatory response syndrome between monomicrobial and polymicrobial Pseudomonas aeruginosa nosocomial bloodstream infections
- PMID: 16259623
- PMCID: PMC1289283
- DOI: 10.1186/1471-2334-5-94
Comparison of the systemic inflammatory response syndrome between monomicrobial and polymicrobial Pseudomonas aeruginosa nosocomial bloodstream infections
Abstract
Background: Some studies of nosocomial bloodstream infection (nBSI) have demonstrated a higher mortality for polymicrobial bacteremia when compared to monomicrobial nBSI. The purpose of this study was to compare differences in systemic inflammatory response and mortality between monomicrobial and polymicrobial nBSI with Pseudomonas aeruginosa.
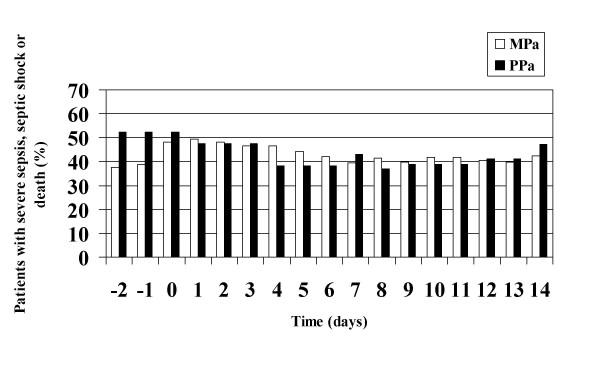
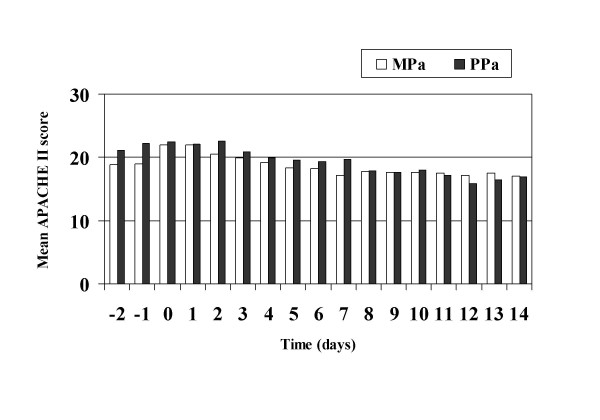
Methods: We performed a historical cohort study on 98 adults with P. aeruginosa (Pa) nBSI. SIRS scores were determined 2 days prior to the first positive blood culture through 14 days afterwards. Monomicrobial (n = 77) and polymicrobial BSIs (n = 21) were compared.
Results: 78.6% of BSIs were caused by monomicrobial P. aeruginosa infection (MPa) and 21.4% by polymicrobial P. aeruginosa infection (PPa). Median APACHE II score on the day of BSI was 22 for MPa and 23 for PPa BSIs. Septic shock occurred in 33.3% of PPa and in 39.0% of MPa (p = 0.64). Progression to septic shock was associated with death more frequently in PPa (OR 38.5, CI95 2.9-508.5) than MPa (OR 4.5, CI95 1.7-12.1). Maximal SIR (severe sepsis, septic shock or death) was seen on day 0 for PPa BSI vs. day 1 for MPa. No significant difference was noted in the incidence of organ failure, 7-day or overall mortality between the two groups. Univariate analysis revealed that APACHE II score > or = 20 at BSI onset, Charlson weighted comorbidity index > or = 3, burn injury and respiratory, cardiovascular, renal and hematologic failure were associated with death, while age, malignant disease, diabetes mellitus, hepatic failure, gastrointestinal complications, inappropriate antimicrobial therapy, infection with imipenem resistant P. aeruginosa and polymicrobial nBSI were not. Multivariate analysis revealed that hematologic failure (p < 0.001) and APACHE II score > or = 20 at BSI onset (p = 0.005) independently predicted death.
Conclusion: In this historical cohort study of nBSI with P. aeruginosa, the incidence of septic shock and organ failure was high in both groups. Additionally, patients with PPa BSI were not more acutely ill, as judged by APACHE II score prior to blood culture positivity than those with MPa BSI. Using multivariable logistic regression analysis, the development of hematologic failure and APACHE II score > or = 20 at BSI onset were independent predictors of death; however, PPa BSI was not.
Figures
Similar articles
-
Systemic inflammatory response syndrome in adult patients with nosocomial bloodstream infection due to Pseudomonas aeruginosa.J Infect. 2006 Jul;53(1):30-5. doi: 10.1016/j.jinf.2005.08.032. Epub 2005 Oct 25. J Infect. 2006. PMID: 16253333
-
Systemic inflammatory response syndrome in adult patients with nosocomial bloodstream infections due to enterococci.BMC Infect Dis. 2006 Sep 26;6:145. doi: 10.1186/1471-2334-6-145. BMC Infect Dis. 2006. PMID: 17002792 Free PMC article.
-
Systemic inflammatory response syndrome in nosocomial bloodstream infections with Pseudomonas aeruginosa and Enterococcus Species: comparison of elderly and nonelderly patients.J Am Geriatr Soc. 2006 May;54(5):804-8. doi: 10.1111/j.1532-5415.2006.00698.x. J Am Geriatr Soc. 2006. PMID: 16696747
-
Rates, predictors and mortality of community-onset bloodstream infections due to Pseudomonas aeruginosa: systematic review and meta-analysis.Clin Microbiol Infect. 2019 Aug;25(8):964-970. doi: 10.1016/j.cmi.2019.04.005. Epub 2019 Apr 14. Clin Microbiol Infect. 2019. PMID: 30995530
-
Short versus prolonged duration of therapy for Pseudomonas aeruginosa bacteraemia: a systematic review and meta-analysis.J Hosp Infect. 2024 Jun;148:155-166. doi: 10.1016/j.jhin.2024.04.007. Epub 2024 Apr 28. J Hosp Infect. 2024. PMID: 38685414
Cited by
-
Gram positive and Gram negative bacteria differ in their sensitivity to cold plasma.Sci Rep. 2016 Dec 9;6:38610. doi: 10.1038/srep38610. Sci Rep. 2016. PMID: 27934958 Free PMC article.
-
Risk Factors for Mortality in Hospitalized Patients with Stenotrophomonas maltophilia Bacteremia.Infect Drug Resist. 2022 Jul 21;15:3881-3886. doi: 10.2147/IDR.S371129. eCollection 2022. Infect Drug Resist. 2022. PMID: 35903579 Free PMC article.
-
Trends in nosocomial bloodstream infections in a burn intensive care unit: an eight-year survey.Ann Burns Fire Disasters. 2010 Jun 30;23(2):88-94. Ann Burns Fire Disasters. 2010. PMID: 21991204 Free PMC article.
-
Influence of carbapenem resistance on mortality of patients with Pseudomonas aeruginosa infection: a meta-analysis.Sci Rep. 2015 Jun 25;5:11715. doi: 10.1038/srep11715. Sci Rep. 2015. PMID: 26108476 Free PMC article.
-
Microbiological analysis of tunneled hemodialysis catheters isolated from patients receiving hemodialysis in Saskatchewan.Future Microbiol. 2024 Sep;19(13):1129-1144. doi: 10.1080/17460913.2024.2359879. Epub 2024 Aug 16. Future Microbiol. 2024. PMID: 39149853 Free PMC article.
References
-
- Pittet D, Li N, Woolson RF, Wenzel RP. Microbiological factors influencing the outcome of nosocomial bloodstream infections: a 6-year validated, population-based model. Clin Infect Dis. 1997;24:1068–1078. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
