

Communication of bed allocation decisions in a critical care unit and accountability for reasonableness
- PMID: 16259634
- PMCID: PMC1298296
- DOI: 10.1186/1472-6963-5-67
Communication of bed allocation decisions in a critical care unit and accountability for reasonableness
Abstract
Background: Communication may affect perceptions of fair process for intensive care unit bed allocation decisions through its impact on the publicity condition of accountability for reasonableness.
Methods: We performed a qualitative case study to describe participant perceptions of the communication of bed allocation decisions in an 18-bed university affiliated, medical-surgical critical care unit at Sunnybrook and Women's College Health Sciences Centre. Interviewed participants were 3 critical care physicians, 4 clinical fellows in critical care, 4 resource nurses, 4 "end-users" (physicians who commonly referred patients to the unit), and 3 members of the administrative staff. Median bed occupancy during the study period (Jan-April 2003) was 18/18; daily admissions and discharges (median) were 3. We evaluated our description using the ethical framework "accountability for reasonableness" (A4R) to identify opportunities for improvement.
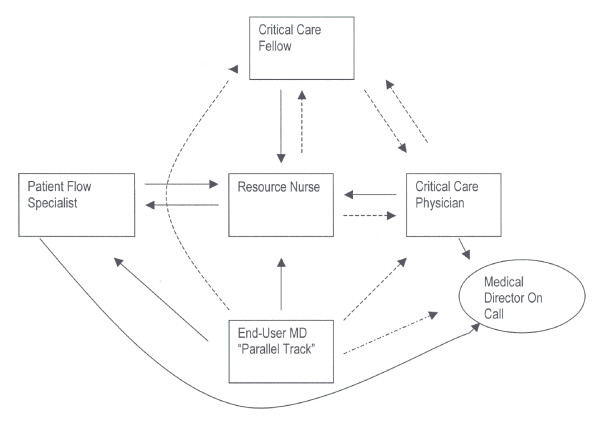
Results: The critical care physician, resource nurse, critical care fellow and end-users (trauma team leader, surgeons, neurosurgeons, anesthesiologists) functioned independently in unofficial "parallel tracks" of bed allocation decision-making; this conflicted with the official designation of the critical care physician as the sole authority. Communication between key decision-makers was indirect and could exclude those affected by the decisions; notably, family members. Participants perceived a lack of publicity for bed allocation rationales.
Conclusion: The publicity condition should be improved for critical care bed allocation decisions. Decision-making in the "parallel tracks" we describe might be unavoidable within usual constraints of time, urgency and demand. Formal guidelines for direct communication between key participants in such circumstances would help to improve the fairness of these decisions.
Figures
References
-
- Anonymous Fair Allocation Of Intensive Care Unit Resources. American Thoracic Society American Journal of Respiratory & Critical Care Medicine. 1997;156:1282–1301. - PubMed
-
- Society of Critical Care Medicine Ethics Committee Consensus Statement On The Triage Of Critically Ill Patients. JAMA. 2004;271:1200–1203. - PubMed
-
- Daniels N, Sabin JE. Setting Limits Fairly: Can We Learn to Share Medical Resources? Oxford, Oxford University Press; 2002.
-
- Mielke J, Martin DK, Singer PA. Priority Setting In A Hospital Critical Care Unit: Qualitative Case Study. Crit Care Med. 2003;31:2764–2768. doi: 10.1097/01.CCM.0000098440.74735.DE. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
