

A meta-analysis of two randomised trials of early chemotherapy in asymptomatic metastatic colorectal cancer
- PMID: 16265352
- PMCID: PMC2361520
- DOI: 10.1038/sj.bjc.6602841
A meta-analysis of two randomised trials of early chemotherapy in asymptomatic metastatic colorectal cancer
Abstract
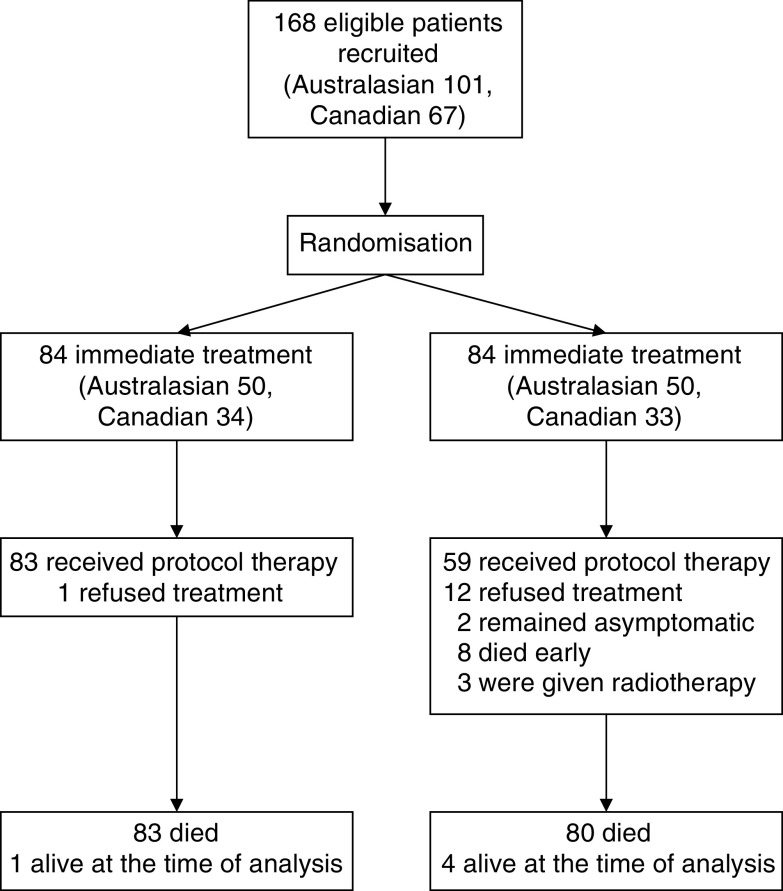
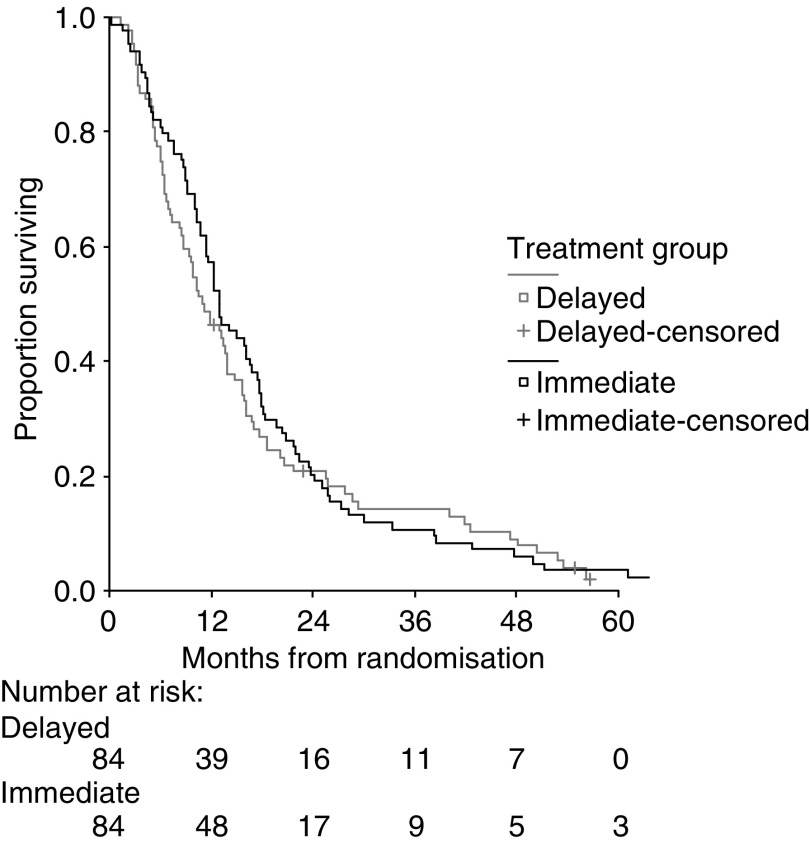
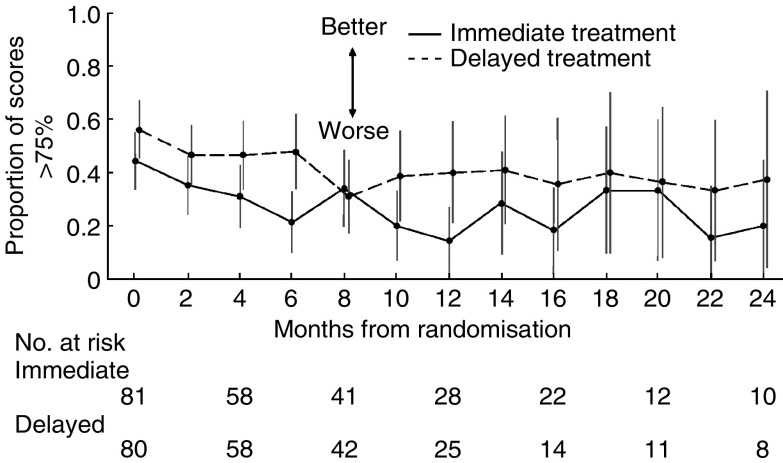
This report constitutes a prospectively planned meta-analysis combining two almost identical trials undertaken in Australasia and Canada to study the effect of starting chemotherapy immediately in asymptomatic patients with metastatic colorectal cancer. Patients (n=168) were randomised to receive either immediate or delayed treatment (at onset of predefined symptoms). Australasian patients received either weekly 5-fluorouracil and leucovorin (500 and 20 mg m(-2), respectively) (n=59) or the daily x 5 Mayo Clinic schedule (425 and 20 mg m(-2), respectively) (n=42). Canadian patients were treated with the Mayo schedule (n=67). Otherwise, the two studies were almost identical in design and each used the European Organisation for the Research and Treatment of Cancer (EORTC) QLQ-C30 instrument for measuring quality of life (QoL). Treatment was continued until 6 months had elapsed or disease progression occurred. Low accrual led to trial suspension before the predetermined sample size for either study was reached. Median survival was not significantly better with immediate treatment (median 13.0 vs 11.0 months; hazard ratio, 1.15; 95% confidence interval (CI) 0.79-1.72; P=0.49). There was no statistically significant difference in progression-free survival (time from randomisation until first evidence of progression after chemotherapy, 10.2 vs 10.8 months; hazard ratio, 1.08; 95% CI 0.71-1.64; P=0.73). There was no difference in overall QoL or its individual domains between the two treatment strategies at baseline or at any subsequent time point. Early treatment of asymptomatic patients with metastatic colorectal cancer did not provide a survival benefit or improved QoL compared to withholding treatment until symptoms occurred.
Figures
References
-
- Aaronson NK, Ahmedzai S, Bergman B (1991) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality of life instrument for use in international trials in oncology. J Natl Cancer Inst 85: 365–376 - PubMed
-
- Buroker TR, O'Connell MJ, Wieand S, Krook JE, Gerstner JB, Mailliard JA, Schaefer PL, Levitt R, Kardinal CG, Gesme Jr DH (1994) Randomized comparison of two schedules of fluorouracil and leucovorin in the treatment of advanced colorectal cancer. J Clin Oncol 12: 14–20 - PubMed
-
- Coates A, Dillenbeck CF, McNeil DR, Kaye SB, Sims K, Fox RM, Woods RL, Milton GW, Solomon J, Tattersall MH (1983) On the receiving end – II. Linear analogue self-assessment (LASA) in evaluation of aspects of the quality of life of cancer patients receiving therapy. Eur J Cancer Clin Oncol 19: 1633–1637 - PubMed
-
- Conroy T, Bleiberg H, Glimelius B (2003) Quality of life in patients with advanced colorectal cancer: what has been learnt? Eur J Cancer 39: 287–294 - PubMed
-
- Glimelius B, Hoffman K, Graf W, Haglund U, Nyren O, Pahlman L, Sjoden PO (1995) Cost-effectiveness of palliative chemotherapy in advanced gastrointestinal cancer. Ann Oncol 6: 267–274 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
