

Cerebrospinal fluid HIV infection and pleocytosis: relation to systemic infection and antiretroviral treatment
- PMID: 16266436
- PMCID: PMC1299327
- DOI: 10.1186/1471-2334-5-98
Cerebrospinal fluid HIV infection and pleocytosis: relation to systemic infection and antiretroviral treatment
Abstract
Background: Central nervous system (CNS) exposure to HIV is a universal facet of systemic infection. Because of its proximity to and shared barriers with the brain, cerebrospinal fluid (CSF) provides a useful window into and model of human CNS HIV infection.
Methods: Prospective study of the relationships of CSF to plasma HIV RNA, and the effects of: 1) progression of systemic infection, 2) CSF white blood cell (WBC) count, 3) antiretroviral therapy (ART), and 4) neurological performance. One hundred HIV-infected subjects were cross-sectionally studied, and 28 were followed longitudinally after initiating or changing ART.
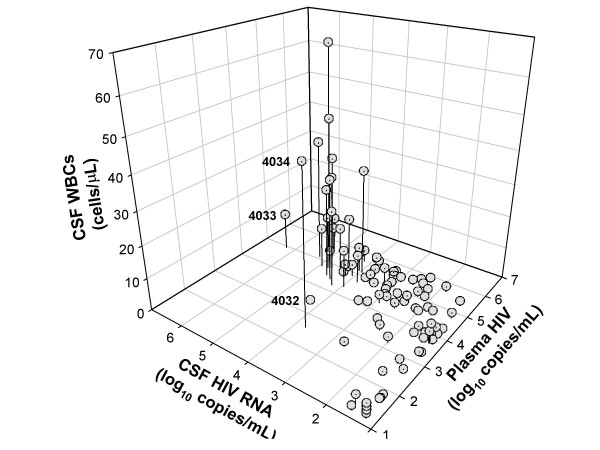
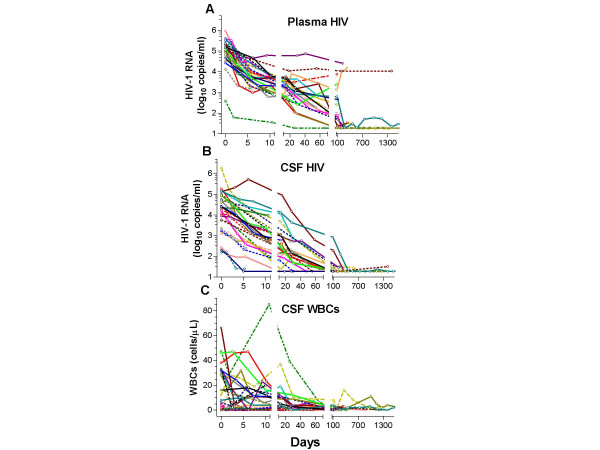
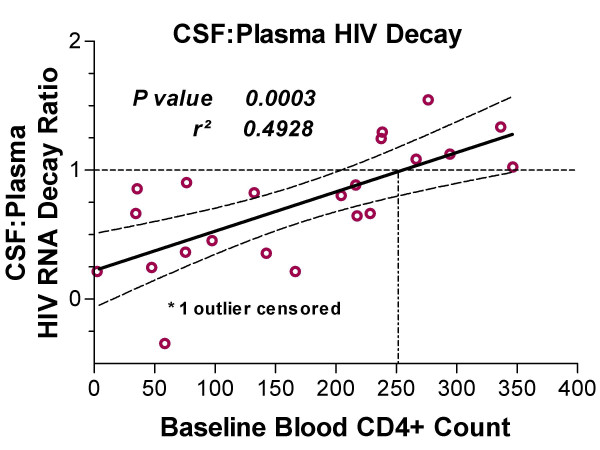
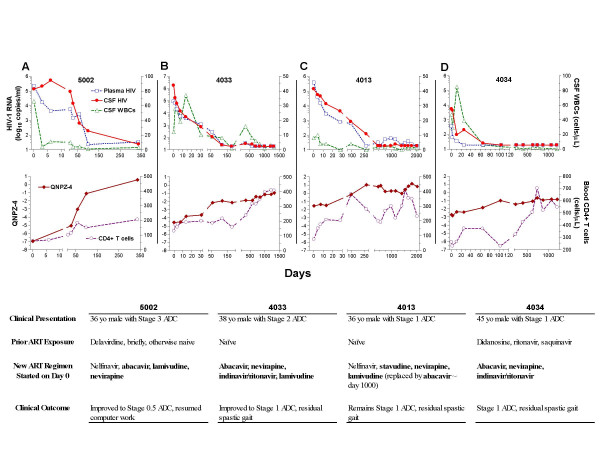
Results: In cross-sectional analysis, HIV RNA levels were lower in CSF than plasma (median difference 1.30 log10 copies/mL). CSF HIV viral loads (VLs) correlated strongly with plasma VLs and CSF WBC counts. Higher CSF WBC counts associated with smaller differences between plasma and CSF HIV VL. CSF VL did not correlate with blood CD4 count, but CD4 counts <50 cells/microL associated with a low prevalence of CSF pleocytosis and large differences between plasma and CSF VL. CSF HIV RNA correlated neither with the severity of the AIDS dementia complex (ADC) nor abnormal quantitative neurological performance, although these measures were associated with depression of CD4 counts. In subjects starting ART, those with lower CD4 counts had slower initial viral decay in CSF than in plasma. In all subjects, including five with persistent plasma viremia and four with new-onset ADC, CSF HIV eventually approached or reached the limit of viral detection and CSF pleocytosis resolved.
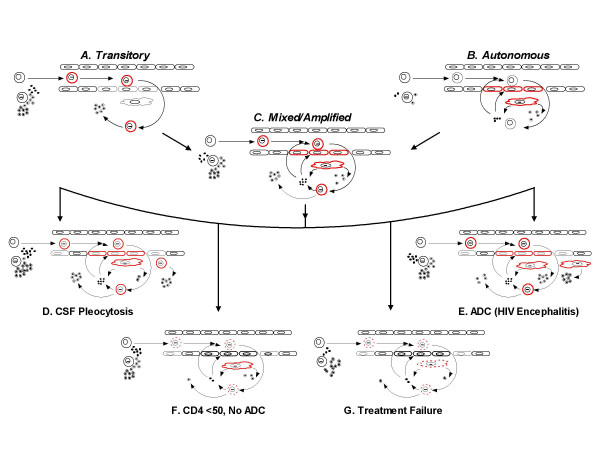
Conclusion: CSF HIV infection is common across the spectrum of infection and is directly related to CSF pleocytosis, though whether the latter is a response to or a contributing cause of CSF infection remains uncertain. Slowing in the rate of CSF response to ART compared to plasma as CD4 counts decline indicates a changing character of CSF infection with systemic immunological progression. Longer-term responses indicate that CSF infection generally responds well to ART, even in the face of systemic virological failure due to drug resistance. We present simple models to explain the differing relationships of CSF to plasma HIV in these settings.
Figures


References
-
- Marshall DW, Brey RL, Cahill WT, Houk RW, Zajac RA, Boswell RN. Spectrum of cerebrospinal fluid findings in various stages of human immunodeficiency virus infection. Arch Neurol. 1988;45:954–958. - PubMed
-
- Brew BJ, Pemberton L, Cunningham P, Law MG. Levels of human immunodeficiency virus type 1 RNA in cerebrospinal fluid correlate with AIDS dementia stage. J Inf Dis. 1997;175:963–966. - PubMed
-
- Pilcher CD, Shugars DC, Fiscus SA, Miller WC, Menezes P, Giner J, Dean B, Robertson K, Hart CE, Lennox JL, Eron JJJ, Hicks CB. HIV in body fluids during primary HIV infection: implications for pathogenesis, treatment and public health. Aids. 2001;15:837–845. doi: 10.1097/00002030-200105040-00004. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
