

Efficiency of 7.2% hypertonic saline hydroxyethyl starch 200/0.5 versus mannitol 15% in the treatment of increased intracranial pressure in neurosurgical patients - a randomized clinical trial [ISRCTN62699180]
- PMID: 16277715
- PMCID: PMC1297608
- DOI: 10.1186/cc3767
Efficiency of 7.2% hypertonic saline hydroxyethyl starch 200/0.5 versus mannitol 15% in the treatment of increased intracranial pressure in neurosurgical patients - a randomized clinical trial [ISRCTN62699180]
Abstract
Introduction: This prospective randomized clinical study investigated the efficacy and safety of 7.2% hypertonic saline hydroxyethyl starch 200/0.5 (7.2% NaCl/HES 200/0.5) in comparison with 15% mannitol in the treatment of increased intracranial pressure (ICP).
Methods: Forty neurosurgical patients at risk of increased ICP were randomized to receive either 7.2% NaCl/HES 200/0.5 or 15% mannitol at a defined infusion rate, which was stopped when ICP was < 15 mmHg.
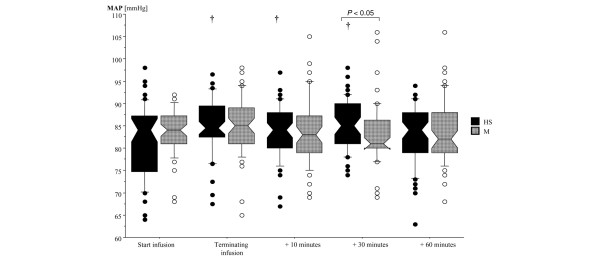
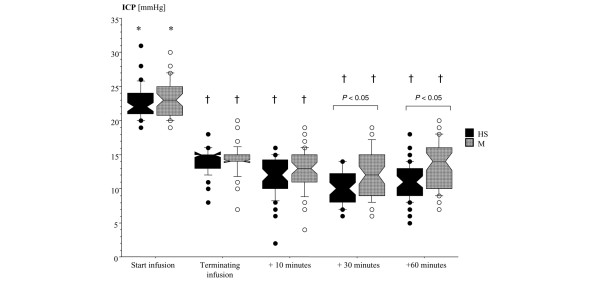
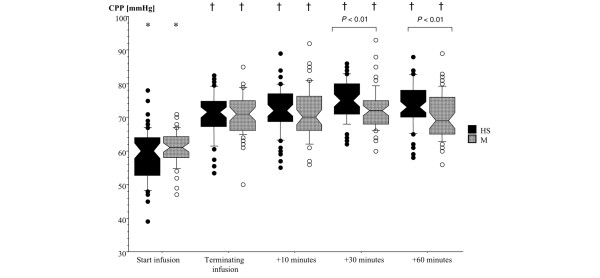
Results: Of the 40 patients, 17 patients received 7.2% NaCl/HES 200/0.5 and 15 received mannitol 15%. In eight patients, ICP did not exceed 20 mmHg so treatment was not necessary. Both drugs decreased ICP below 15 mmHg (p < 0.0001); 7.2% NaCl/HES 200/0.5 within 6.0 (1.2-15.0) min (all results are presented as median (minimum-maximum range)) and mannitol within 8.7 (4.2-19.9) min (p < 0.0002). 7.2% NaCl/HES 200/0.5 caused a greater decrease in ICP than mannitol (57% vs 48%; p < 0.01). The cerebral perfusion pressure was increased from 60 (39-78) mmHg to 72 (54-85) mmHg by infusion with 7.2% NaCl/HES 200/0.5 (p < 0.0001) and from 61 (47-71) mmHg to 70 (50-79) mmHg with mannitol (p < 0.0001). The mean arterial pressure was increased by 3.7% during the infusion of 7.2% NaCl/HES 200/0.5 but was not altered by mannitol. There were no clinically relevant effects on electrolyte concentrations and osmolarity in the blood. The mean effective dose to achieve an ICP below 15 mmHg was 1.4 (0.3-3.1) ml/kg for 7.2% NaCl/HES 200/0.5 and 1.8 (0.45-6.5) ml/kg for mannitol (p < 0.05).
Conclusion: 7.2% NaCl/HES 200/0.5 is more effective than mannitol 15% in the treatment of increased ICP. A dose of 1.4 ml/kg of 7.2% NaCl/HES 200/0.5 can be recommended as effective and safe. The advantage of 7.2% NaCl/HES 200/0.5 might be explained by local osmotic effects, because there were no clinically relevant differences in hemodynamic clinical chemistry parameters.
Figures
References
-
- Lang EW, Chesnut RM. Intracranial pressure and cerebral perfusion pressure in severe head injury. New Horiz. 1995;3:400–409. - PubMed
-
- Chesnut RM. Medical management of severe head injury: present and future. New Horiz. 1995;3:581–593. - PubMed
-
- Procaccio F, Stocchetti N, Citerio G, Berardino M, Beretta L, Della Corte F, D'Avella D, Brambilla GL, Delfini R, Servadei F, Tomei G. Guidelines for the treatment of adults with severe head trauma (part II). Criteria for medical treatment. J Neurosurg Sci. 2000;44:11–18. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
