

Hospital-acquired sinusitis is a common cause of fever of unknown origin in orotracheally intubated critically ill patients
- PMID: 16277722
- PMCID: PMC1297630
- DOI: 10.1186/cc3805
Hospital-acquired sinusitis is a common cause of fever of unknown origin in orotracheally intubated critically ill patients
Abstract
Introduction: Sinusitis is a well recognised but insufficiently understood complication of critical illness. It has been linked to nasotracheal intubation, but its occurrence after orotracheal intubation is less clear. We studied the incidence of sinusitis in patients with fever of unknown origin (FUO) in our intensive care unit with the aim of establishing a protocol that would be applicable in everyday clinical practice.
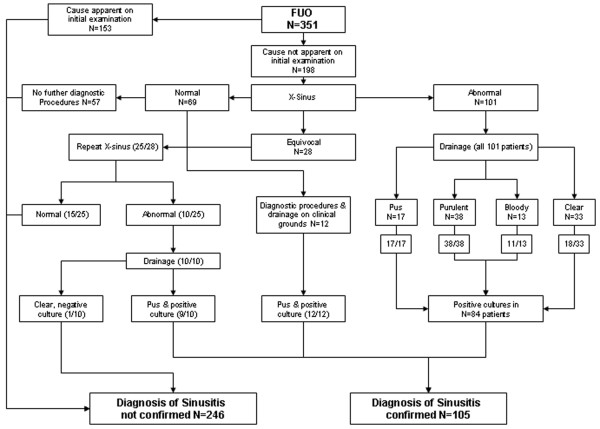
Methods: Sinus X-rays (SXRs) were performed in all patients with fever for which an initial screening (physical examination, microbiological cultures and chest X-ray) revealed no obvious cause. All patients were followed with a predefined protocol, including antral drainage in all patients with abnormal or equivocal results on their SXR.
Results: Initial screening revealed probable causes of fever in 153 of 351 patients (43.6%). SXRs were taken in the other 198 patients (56.4%); 129 had obvious or equivocal abnormalities. Sinus drainage revealed purulent material and positive cultures (predominantly Pseudomonas and Klebsiella species) in 84 patients. Final diagnosis for the cause of fever in all 351 patients based on X-ray results, microbiological cultures, and clinical response to sinus drainage indicated sinusitis as the sole cause of fever in 57 (16.2%) and as contributing factor in 48 (13.8%) patients with FUO. This will underestimate the actual incidence because SXR and drainage were not performed in all patients.
Conclusion: Physicians treating critically ill patients should be aware of the high risk of sinusitis and take appropriate preventive measures, including the removal of nasogastric tubes in patients requiring long-term mechanical ventilation. Routine investigation of FUO should include computed tomography scan, SXR or sinus ultrasonography, and drainage should be performed if any abnormalities are found.
Figures
Similar articles
-
[Sinusitis in long-term intubated, intensive care patients: nasal versus oral intubation].Anaesthesist. 1991 Feb;40(2):100-4. Anaesthesist. 1991. PMID: 2048700 Clinical Trial. German.
-
Sinusitis in the critical care patient.New Horiz. 1993 May;1(2):261-70. New Horiz. 1993. PMID: 7522919 Review.
-
Value of antral puncture in the intensive care patient with fever of unknown origin.Laryngoscope. 2000 Oct;110(10 Pt 1):1702-6. doi: 10.1097/00005537-200010000-00025. Laryngoscope. 2000. PMID: 11037829
-
[Sinusitis during intensive care. Prospective studies].Ann Otolaryngol Chir Cervicofac. 1990;107(5):329-32. Ann Otolaryngol Chir Cervicofac. 1990. PMID: 2221727 French.
-
[Sinusitis during nasotracheal intubation].Rev Laryngol Otol Rhinol (Bord). 1989;110(1):93-6. Rev Laryngol Otol Rhinol (Bord). 1989. PMID: 2491725 Review. French.
Cited by
-
Infectious causes of fever of unknown origin in developing countries: An international ID-IRI study.J Intensive Med. 2023 Sep 28;4(1):94-100. doi: 10.1016/j.jointm.2023.07.004. eCollection 2024 Jan. J Intensive Med. 2023. PMID: 38263972 Free PMC article.
-
Systemic inflammation response index predicts the postoperative recurrence of chronic rhinosinusitis with nasal polyps: a retrospective study in the Chinese population.Eur Arch Otorhinolaryngol. 2024 Jan;281(1):207-217. doi: 10.1007/s00405-023-08182-8. Epub 2023 Aug 17. Eur Arch Otorhinolaryngol. 2024. PMID: 37589753
-
[Nosocomial sinusitis in an intensive care unit: a microbiological study].Braz J Otorhinolaryngol. 2011 Jan-Feb;77(1):102-6. doi: 10.1590/S1808-86942011000100017. Braz J Otorhinolaryngol. 2011. PMID: 21340197 Free PMC article.
-
Comparison of nasotracheal versus orotracheal intubation for sedation, assisted spontaneous breathing, mobilization, and outcome in critically ill patients: an exploratory retrospective analysis.Sci Rep. 2023 Aug 3;13(1):12616. doi: 10.1038/s41598-023-39768-1. Sci Rep. 2023. PMID: 37537207 Free PMC article.
-
The role of maxillary sinus puncture on the diagnosis and treatment of patients with hospital-acquired rhinosinusitis.Braz J Otorhinolaryngol. 2012 Jul-Aug;78(4):35-41. doi: 10.1590/S1808-86942012000400008. Braz J Otorhinolaryngol. 2012. PMID: 22936134 Free PMC article.
References
-
- Chastre J, Fagon J. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165:867–903. - PubMed
-
- Anon Hospital-acquired pneumonia in adults: diagnosis, assessment of severity, initial antimicrobial therapy, and preventive strategies. A consensus statement. American Thoracic Society, November 1995. Am J Respir Crit Care Med. 1996;153:1711–1725. - PubMed
-
- O'Grady NP, Alexander M, Dellinger EP, Gerberding JL, Heard SO, Maki DG, Masur H, McCormick RD, Mermel LA, Pearson ML, et al. Guidelines for the prevention of intravascular catheter-related infections. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2002;51:1–29. - PubMed
-
- Bach A, Boehrer H, Schmidt H, Geiss HK. Nosocomial sinusitis in ventilated patients. Nasotracheal versus orotracheal intubation. Anaesthesia. 1992;47:335–339. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
