

Bench-to-bedside review: oxygen debt and its metabolic correlates as quantifiers of the severity of hemorrhagic and post-traumatic shock
- PMID: 16277731
- PMCID: PMC1297598
- DOI: 10.1186/cc3526
Bench-to-bedside review: oxygen debt and its metabolic correlates as quantifiers of the severity of hemorrhagic and post-traumatic shock
Abstract
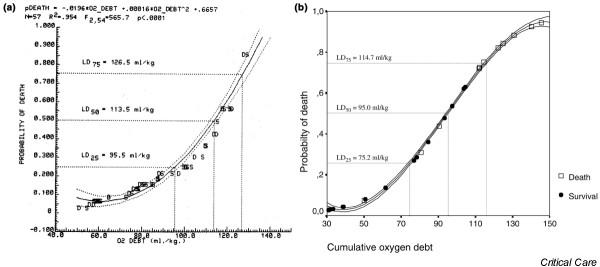
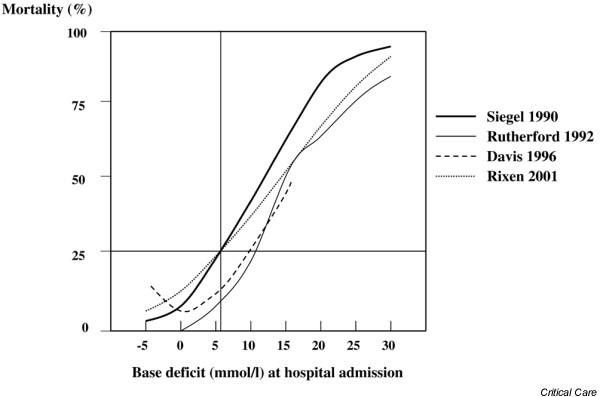
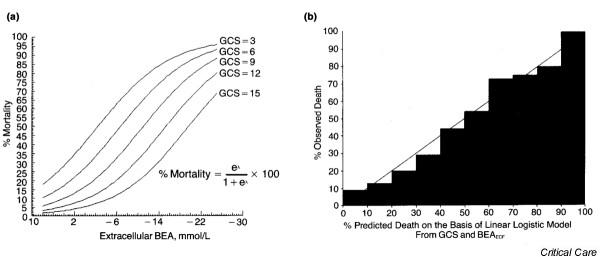
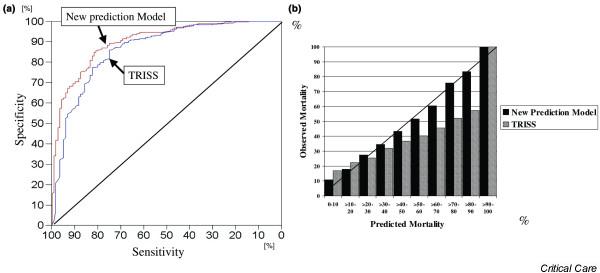
Evidence is increasing that oxygen debt and its metabolic correlates are important quantifiers of the severity of hemorrhagic and post-traumatic shock and and may serve as useful guides in the treatment of these conditions. The aim of this review is to demonstrate the similarity between experimental oxygen debt in animals and human hemorrhage/post-traumatic conditions, and to examine metabolic oxygen debt correlates, namely base deficit and lactate, as indices of shock severity and adequacy of volume resuscitation. Relevant studies in the medical literature were identified using Medline and Cochrane Library searches. Findings in both experimental animals (dog/pig) and humans suggest that oxygen debt or its metabolic correlates may be more useful quantifiers of hemorrhagic shock than estimates of blood loss, volume replacement, blood pressure, or heart rate. This is evidenced by the oxygen debt/probability of death curves for the animals, and by the consistency of lethal dose (LD)25,50 points for base deficit across all three species. Quantifying human post-traumatic shock based on base deficit and adjusting for Glasgow Coma Scale score, prothrombin time, Injury Severity Score and age is demonstrated to be superior to anatomic injury severity alone or in combination with Trauma and Injury Severity Score. The data examined in this review indicate that estimates of oxygen debt and its metabolic correlates should be included in studies of experimental shock and in the management of patients suffering from hemorrhagic shock.
Figures
References
-
- Siegel JH, Linberg SE, Wiles CE. Therapy of low-flow shock states. In: Siegel JH, editor. Trauma: Emergency Surgery and Critical Care. Churchill Livingston: New York; 1987. pp. 201–284.
-
- Siegel JH. Through a glass darkly: the lung as a window to monitor oxygen consumption, energy metabolism, and severity of critical illness. Clin Chem. 1990;36:1585–1593. - PubMed
-
- American College of Surgeons . Advanced Trauma Life Support Manual. American College of Surgeons; 1997. Shock; pp. 87–108.
-
- Crowell JW, Smith EE. Oxygen deficit and irreversible hemorrhagic shock. Am J Physiol. 1964;206:313–316. - PubMed
-
- Rush BF, Rosenberg JC, Spencer FC. Changes in oxygen consumption in shock. J Surg Res. 1965;5:252–255. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
