

Clinical review: respiratory mechanics in spontaneous and assisted ventilation
- PMID: 16277736
- PMCID: PMC1297597
- DOI: 10.1186/cc3516
Clinical review: respiratory mechanics in spontaneous and assisted ventilation
Abstract
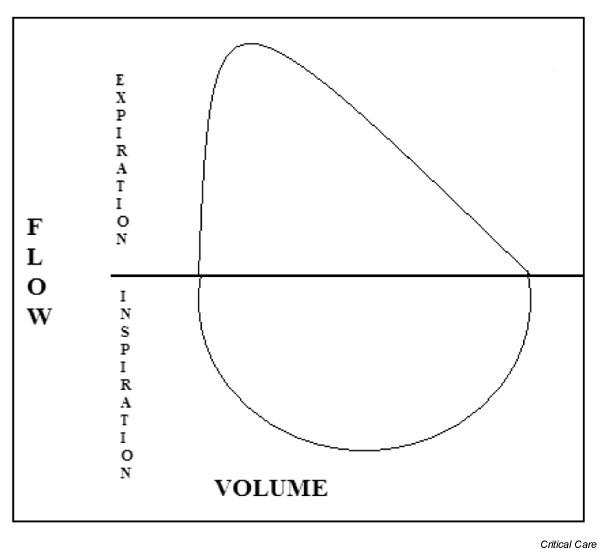
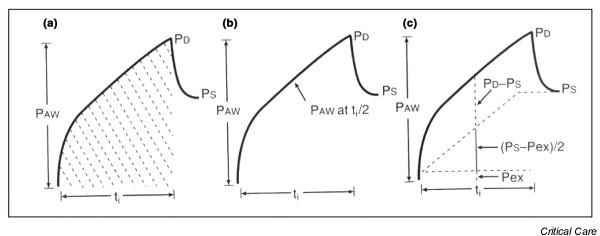
Pulmonary disease changes the physiology of the lungs, which manifests as changes in respiratory mechanics. Therefore, measurement of respiratory mechanics allows a clinician to monitor closely the course of pulmonary disease. Here we review the principles of respiratory mechanics and their clinical applications. These principles include compliance, elastance, resistance, impedance, flow, and work of breathing. We discuss these principles in normal conditions and in disease states. As the severity of pulmonary disease increases, mechanical ventilation can become necessary. We discuss the use of pressure-volume curves in assisting with poorly compliant lungs while on mechanical ventilation. In addition, we discuss physiologic parameters that assist with ventilator weaning as the disease process abates.
Figures




References
-
- Truwit JD. Lung mechanics. In: Dantzer DR, MacIntyre NR, Bakow ED, editor. Comprehensive Respiratory Care. Philadelphia: WB Saunders Co; 1995. pp. 18–31.
-
- Costanzo LS. Physiology. 2. Philadelphia: WB Saunders Co; 2002.
-
- Mehta S, Stewart TE, MacDonald R, Hallett D, Banayan D, Lapinsky S, Slutsky A. Temporal change, reproducibility, and inter-observer variability in pressure-volume curves in adults with acute lung injury and acute respiratory distress syndrome. Crit Care Med. 2003;31:2118–2125. doi: 10.1097/01.CCM.0000069342.00360.9F. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
