

Robust nonrigid registration to capture brain shift from intraoperative MRI
- PMID: 16279079
- PMCID: PMC2042023
- DOI: 10.1109/TMI.2005.856734
Robust nonrigid registration to capture brain shift from intraoperative MRI
Abstract
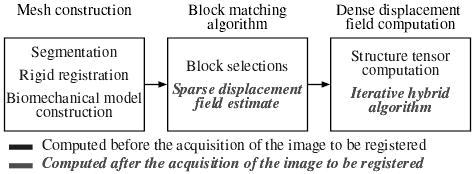
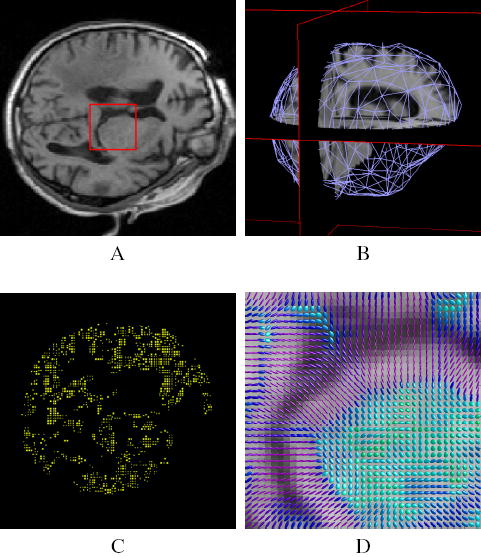
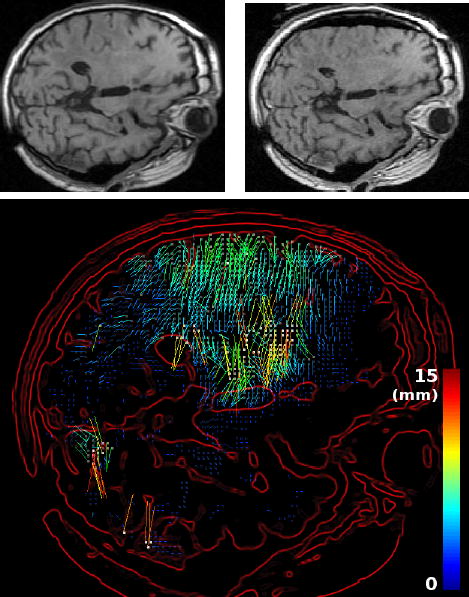
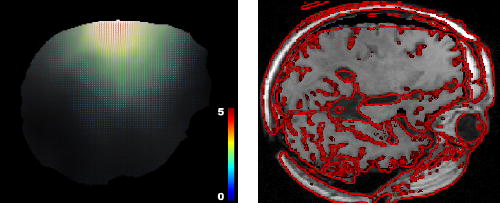
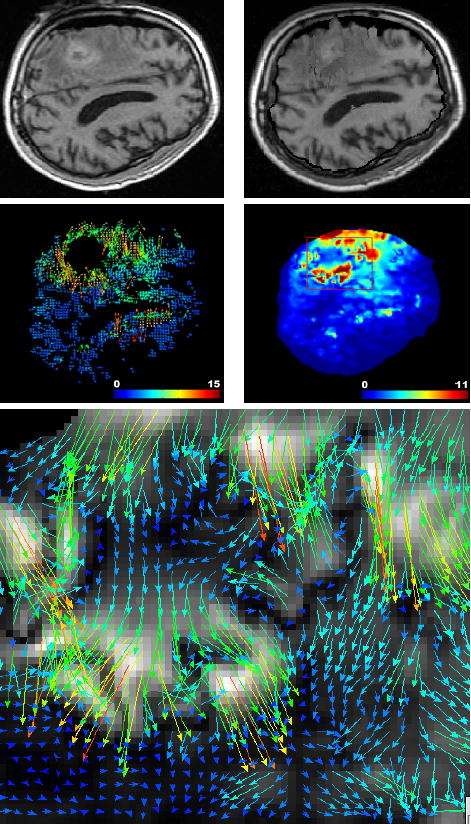
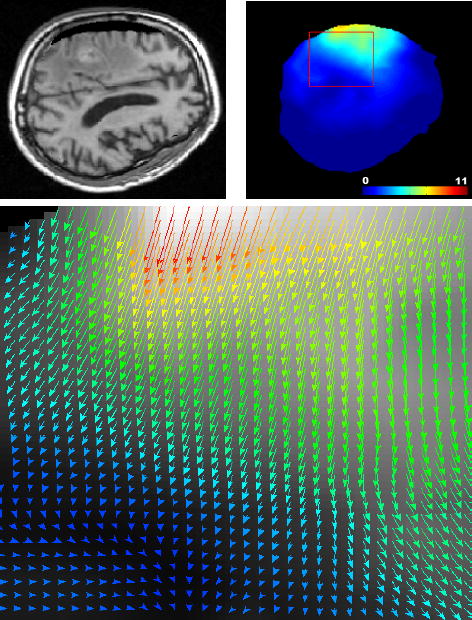
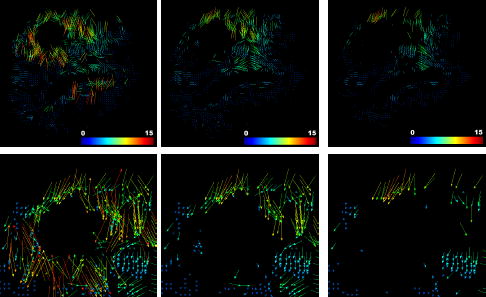
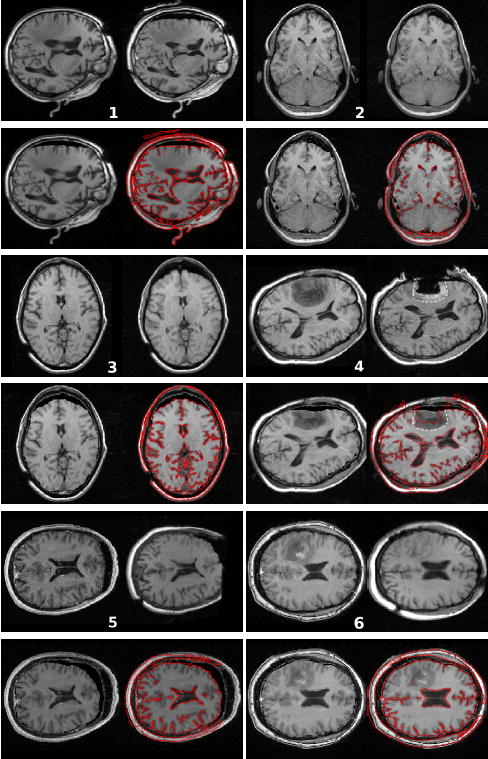
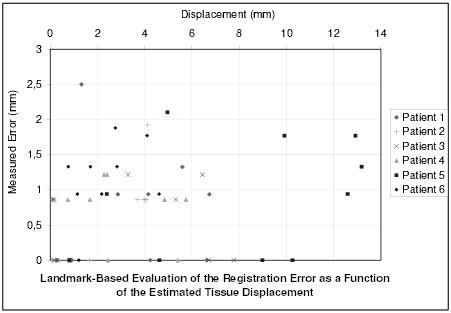
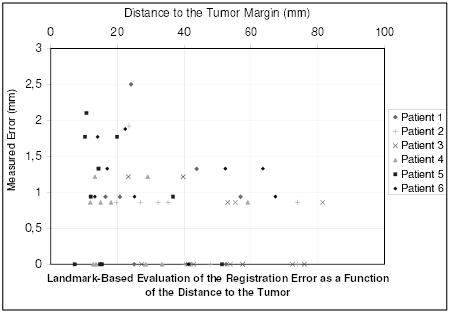
We present a new algorithm to register 3-D preoperative magnetic resonance (MR) images to intraoperative MR images of the brain which have undergone brain shift. This algorithm relies on a robust estimation of the deformation from a sparse noisy set of measured displacements. We propose a new framework to compute the displacement field in an iterative process, allowing the solution to gradually move from an approximation formulation (minimizing the sum of a regularization term and a data error term) to an interpolation formulation (least square minimization of the data error term). An outlier rejection step is introduced in this gradual registration process using a weighted least trimmed squares approach, aiming at improving the robustness of the algorithm. We use a patient-specific model discretized with the finite element method in order to ensure a realistic mechanical behavior of the brain tissue. To meet the clinical time constraint, we parallelized the slowest step of the algorithm so that we can perform a full 3-D image registration in 35 s (including the image update time) on a heterogeneous cluster of 15 personal computers. The algorithm has been tested on six cases of brain tumor resection, presenting a brain shift of up to 14 mm. The results show a good ability to recover large displacements, and a limited decrease of accuracy near the tumor resection cavity.
Figures

References
-
- Kacher D, Maier S, Mamata H, Nabavi YMA, Jolesz F. Motion robust imaging for continuous intraoperative mri. J Magn Reson Imaging. 2001 January;1(13):158–61. - PubMed
-
- Jolesz F. Image-guided procedures and the operating room of the future. Radiology. 1997 May;204(3):601–612. - PubMed
-
- Grimson E, Kikinis R, Jolesz F, Black P. Image-guided surgery. Scientific American. 1999 June;280(6):62–69. - PubMed
-
- Platenik L, Miga M, Roberts D, Lunn K, Kennedy F, Hartov A, Paulsen K. In vivo quantification of retraction deformation modeling for updated image-guidance during neurosurgery. IEEE Transaction on Biomedical Engineering. 2002 August;49(8):823–35. - PubMed
-
- Nimsky C, Ganslandt O, Cerny S, Hastreiter P, Greiner G, Fahlbusch R. Quantification of, visualization of, and compensation for brain shift using intraoperative magnetic resonance imaging. Neurosurgery. 2000 November;47(5):1070–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
