

Early hemoperfusion with an immobilized polymyxin B fiber column eliminates humoral mediators and improves pulmonary oxygenation
- PMID: 16280061
- PMCID: PMC1414001
- DOI: 10.1186/cc3815
Early hemoperfusion with an immobilized polymyxin B fiber column eliminates humoral mediators and improves pulmonary oxygenation
Abstract
Introduction: The objective of this study was to clarify the efficacy and mechanism of action of direct hemoperfusion with an immobilized polymyxin B fiber column (DHP-PMX) in patients with acute lung injury or acute respiratory distress syndrome caused by sepsis.
Method: Thirty-six patients with sepsis were included. In each patient a thermodilution catheter was inserted, and the oxygen delivery index and oxygen consumption index were measured. DHP-PMX was performed in patients with a normal oxygen delivery index and oxygen consumption index (> 500 ml/minute per m2 and > 120 ml/minute per m2, respectively). The Acute Physiology and Chronic Health Evaluation II score was used as an index of the severity of sepsis, and survival was assessed after 1 month. The humoral mediators measured were the chemokine IL-8, plasminogen activator inhibitor-1, and neutrophil elastase (NE). These mediators were measured before DHP-PMX treatment, and at 24, 48, and 78 hours after the start of treatment. The arterial oxygen tension (PaO2)/fractional inspired oxygen (FiO2) ratio was measured before DHP-PMX treatment and at 24, 48, 72, 92, and 120 hours after the start of treatment.
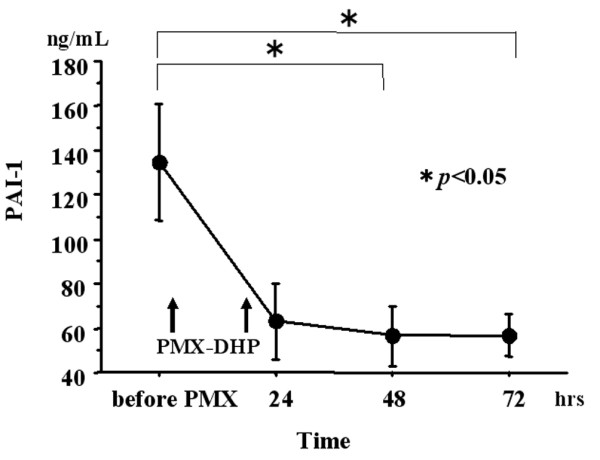
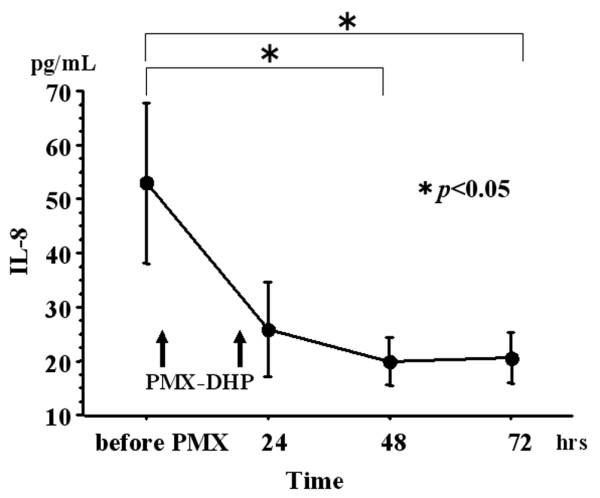
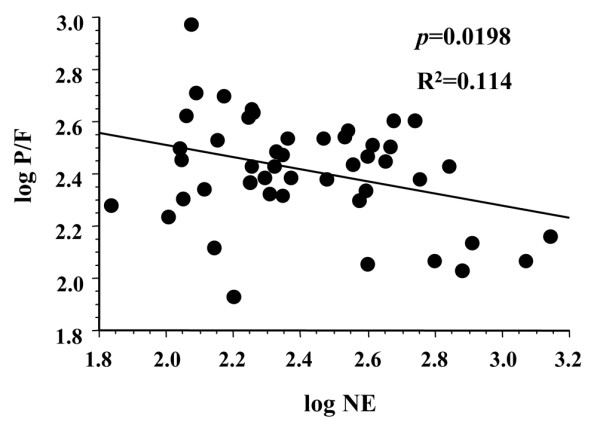
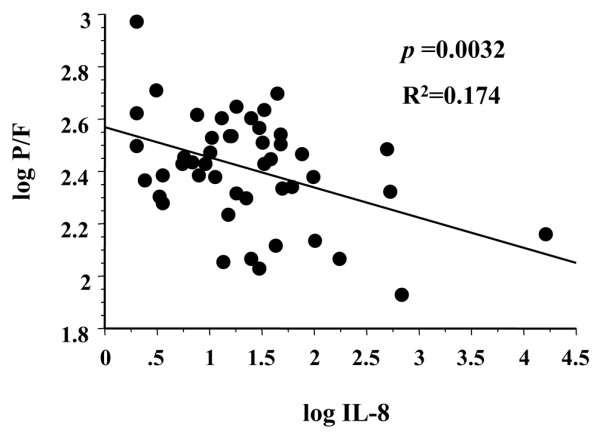
Results: All patients remained alive after 1 month. Before DHP-PMX treatment, the Acute Physiology and Chronic Health Evaluation II score was 24 +/- 2.0, the IL-8 level was 54 +/- 15.8 pg/ml, plasminogen activator inhibitor-1 was 133 +/- 28.1 ng/ml, and NE was 418 +/- 72.1 mug/l. These three humoral mediators began to decrease from 24 hours after DHP-PMX treatment, and the decline became significant from 48 hours onward. The PaO2/FiO2 ratio was 244 +/- 26.3 before DHP-PMX treatment but improved significantly from 96 hours onward. There were significant negative correlations between the PaO2/FiO2 ratio and blood levels of NE and IL-8.
Conclusion: The mechanism of action of DHP-PMX is still not fully understood, but we report the following findings. The mean blood levels of plasminogen activator inhibitor-1, NE, and IL-8 were significantly decreased from 48 hours after DHP-PMX treatment. The mean PaO2/FiO2 ratio was significantly improved from 96 hours after DHP-PMX treatment. Improvement in the PaO2/FiO2 ratio appeared to be related to the decreases in blood NE and IL-8 levels.
Figures


Comment in
-
The place of early haemoperfusion with polymyxin B fibre column in the treatment of sepsis.Crit Care. 2005;9(6):631-3. doi: 10.1186/cc3890. Epub 2005 Oct 18. Crit Care. 2005. PMID: 16356251 Free PMC article.
Similar articles
-
Efficacy of direct hemoperfusion using polymyxin B-immobilized fiber column (PMX-DHP) in rapidly progressive interstitial pneumonias: results of a historical control study and a review of previous studies.Ther Adv Respir Dis. 2017 Jul;11(7):261-275. doi: 10.1177/1753465817708950. Epub 2017 May 30. Ther Adv Respir Dis. 2017. PMID: 28554260 Free PMC article. Review.
-
Hemoperfusion with an immobilized polymyxin B fiber column inhibits activation of vascular endothelial cells.Ther Apher Dial. 2005 Aug;9(4):303-7. doi: 10.1111/j.1744-9987.2005.00286.x. Ther Apher Dial. 2005. PMID: 16076371
-
Impact of Extended Duration of Polymyxin B-Immobilized Fiber Column Direct Hemoperfusion on Hemodynamics, Vasoactive Substance Requirement, and Pulmonary Oxygenation in Patients with Sepsis: An Observational Study.Blood Purif. 2022;51(1):62-69. doi: 10.1159/000515685. Epub 2021 Apr 28. Blood Purif. 2022. PMID: 33910191
-
Treatment of acute exacerbation of idiopathic pulmonary fibrosis with direct hemoperfusion using a polymyxin B-immobilized fiber column improves survival.BMC Pulm Med. 2015 Feb 22;15:15. doi: 10.1186/s12890-015-0004-4. BMC Pulm Med. 2015. PMID: 25887940 Free PMC article.
-
New trends in polymyxin B hemoperfusion: from 2006 to 2013.Blood Purif. 2014;37 Suppl 1:9-13. doi: 10.1159/000356986. Epub 2014 Jan 20. Blood Purif. 2014. PMID: 24457489 Review.
Cited by
-
A systematic review of the efficacy of direct hemoperfusion with a polymyxin B-immobilized fibre column to treat rapidly progressive interstitial pneumonia.SAGE Open Med. 2019 Jul 8;7:2050312119861821. doi: 10.1177/2050312119861821. eCollection 2019. SAGE Open Med. 2019. PMID: 31312451 Free PMC article.
-
Survival from an Acute Exacerbation of Idiopathic Pulmonary Fibrosis with or without Direct Hemoperfusion with a Polymyxin B-immobilized Fiber Column: A Retrospective Analysis.Intern Med. 2016;55(24):3551-3559. doi: 10.2169/internalmedicine.55.6056. Epub 2016 Dec 15. Intern Med. 2016. PMID: 27980253 Free PMC article.
-
Immunomodulation in sepsis: the role of endotoxin removal by polymyxin B-immobilized cartridge.Mediators Inflamm. 2013;2013:507539. doi: 10.1155/2013/507539. Epub 2013 Oct 22. Mediators Inflamm. 2013. PMID: 24249974 Free PMC article. Review.
-
Septic shock from descending necrotizing mediastinitis - combined treatment with IgM-enriched immunoglobulin preparation and direct polymyxin B hemoperfusion: a case report.J Med Case Rep. 2018 Mar 3;12(1):55. doi: 10.1186/s13256-018-1611-5. J Med Case Rep. 2018. PMID: 29499757 Free PMC article.
-
Efficacy of direct hemoperfusion using polymyxin B-immobilized fiber column (PMX-DHP) in rapidly progressive interstitial pneumonias: results of a historical control study and a review of previous studies.Ther Adv Respir Dis. 2017 Jul;11(7):261-275. doi: 10.1177/1753465817708950. Epub 2017 May 30. Ther Adv Respir Dis. 2017. PMID: 28554260 Free PMC article. Review.
References
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RMH, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Conensus Conference Committee. American College of Chest Physicans/Society of Critical Care Medicine. Chest. 1992;101:1644–1655. - PubMed
-
- Ziegler EJ, Fisher CJ, Jnr, Sprung CL, Staraube RC, Sadoff JC, Foulke GE, Wortel CH, Fink MP, Dellinger RP, Teng NNH, et al. Treatment of gram-negative bacteremia and shock with HA-1A human monoclonal antibody against endotoxin. A randomized, double-blind, placebo-controlled trial. The HA-1A Sepsis Study Group. N Engl J Med. 1991;324:429–436. - PubMed
-
- Greenman RL, Schein RMH, Martin MA, Wenzel RP, Macintyre NR, Emmanuel G, Chmel H, Kohler RB, McCarthy M, Plouffe J, et al. A controlled clinical trial of E5 murine monoclonal IgM antibody to endotoxin in the treatment of gram-negative sepsis. The XOMA Sepsis Study Group. JAMA. 1991;266:1097–1102. doi: 10.1001/jama.266.8.1097. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
