

The use of prophylactic fluconazole in immunocompetent high-risk surgical patients: a meta-analysis
- PMID: 16280069
- PMCID: PMC1414000
- DOI: 10.1186/cc3883
The use of prophylactic fluconazole in immunocompetent high-risk surgical patients: a meta-analysis
Abstract
Introduction: High-risk surgical patients are at increased risk of fungal infections and candidaemia. Evidence from observational and small randomised controlled studies suggests that prophylactic fluconazole may be effective in reducing fungal infection and mortality. We evaluated the effects of prophylactic fluconazole on the incidence of candidaemia and hospital mortality in immunocompetent high-risk surgical patients.
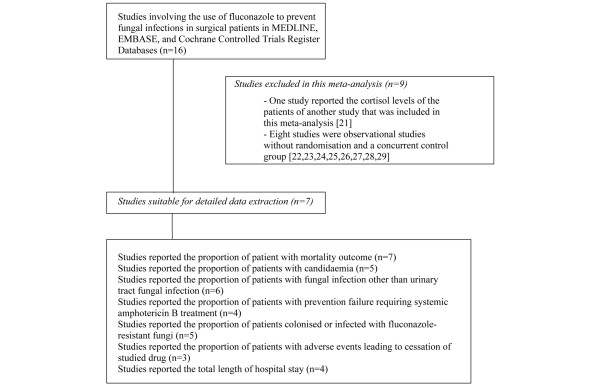
Methods: Randomised controlled studies involving the use of fluconazole in immunocompetent high-risk surgical patients from the Cochrane Controlled Trial Register (2005, issue 1) and from the EMBASE and MEDLINE databases (1966-30 April 2005), without any language restriction, were included. Two reviewers reviewed the quality of the studies and performed data extraction independently.
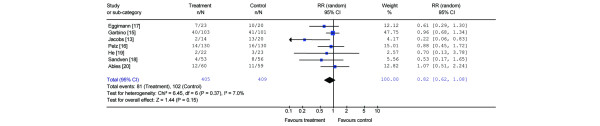
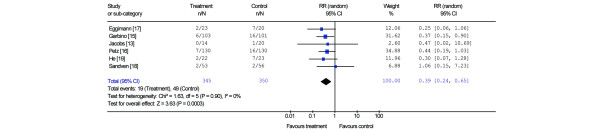
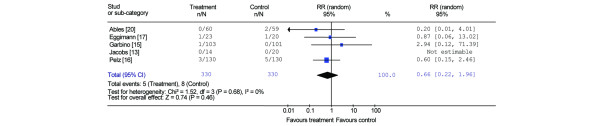
Results: Seven randomised controlled studies with a total of 814 immunocompetent high-risk surgical patients were considered. The use of prophylactic fluconazole was associated with a reduction in the proportion of patients with candidaemia (relative risk [RR] = 0.21, 95% confidence interval [CI] = 0.06-0.72, P = 0.01; I2 = 0%) and fungal infections other than lower urinary tract infection (RR = 0.39, 95% CI = 0.24-0.65, P = 0.0003; I2 = 0%), but was associated with only a trend towards a reduction in hospital mortality (RR = 0.82, 95% CI = 0.62-1.08, P = 0.15; I2 = 7%). The proportion of patients requiring systemic amphotericin B as a rescue therapy for systemic fungal infection was lower after prophylactic use of fluconazole (RR = 0.35, 95% CI = 0.17-0.72, P = 0.004; I2 = 0%). The proportion of patients colonised with or infected with fluconazole-resistant fungi was not significantly different between the fluconazole group and the placebo group (RR = 0.66, 95% CI = 0.22-1.96, P = 0.46; I2 = 0%).
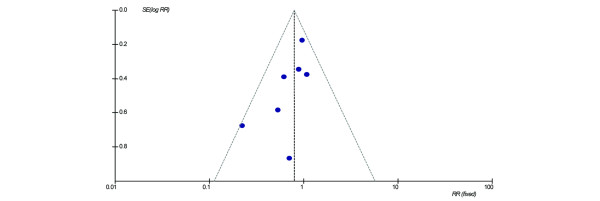
Conclusion: The use of prophylactic fluconazole in immunocompetent high-risk surgical patients is associated with a reduced incidence of candidaemia but with only a trend towards a reduction in hospital mortality.
Figures

Comment in
-
Use of prophylactic fluconazole in a neonatal intensive care unit: efficacy is similar to that described in adult high-risk surgical patients.Crit Care. 2006 Feb;10(1):402. doi: 10.1186/cc3958. Crit Care. 2006. PMID: 16420658 Free PMC article. No abstract available.
References
-
- Tufano R. Focus on risk factors for fungal infections in ICU patients. Minerva Anestesiol. 2002;68:269–272. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
