

Actuarial survival of a large Canadian cohort of preterm infants
- PMID: 16280080
- PMCID: PMC1315360
- DOI: 10.1186/1471-2431-5-40
Actuarial survival of a large Canadian cohort of preterm infants
Abstract
Background: The increased survival of preterm and very low birth weight infants in recent years has been well documented but continued surveillance is required in order to monitor the effects of new therapeutic interventions. Gestation and birth weight specific survival rates most accurately reflect the outcome of perinatal care. Our aims were to determine survival to discharge for a large Canadian cohort of preterm infants admitted to the neonatal intensive care unit (NICU), and to examine the effect of gender on survival and the effect of increasing postnatal age on predicted survival.
Methods: Outcomes for all 19,507 infants admitted to 17 NICUs throughout Canada between January 1996 and October 1997 were collected prospectively. Babies with congenital anomalies were excluded from the study population. Gestation and birth weight specific survival for all infants with birth weight < 1,500 g (n = 3419) or gestation < or = 30 weeks (n = 3119) were recorded. Actuarial survival curves were constructed to show changes in expected survival with increasing postnatal age.
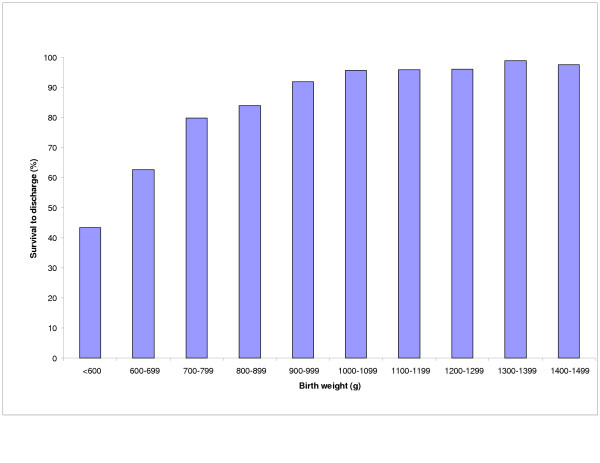
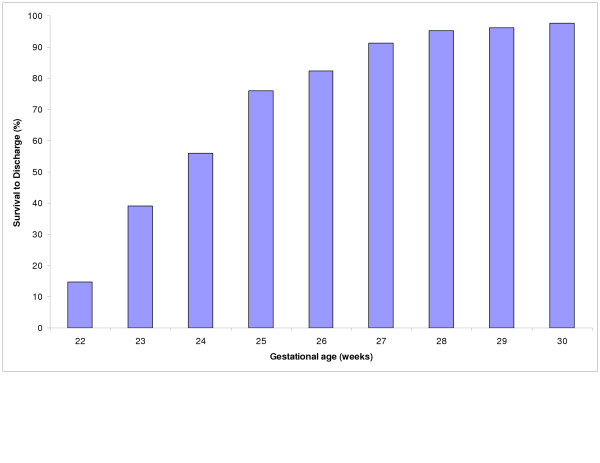
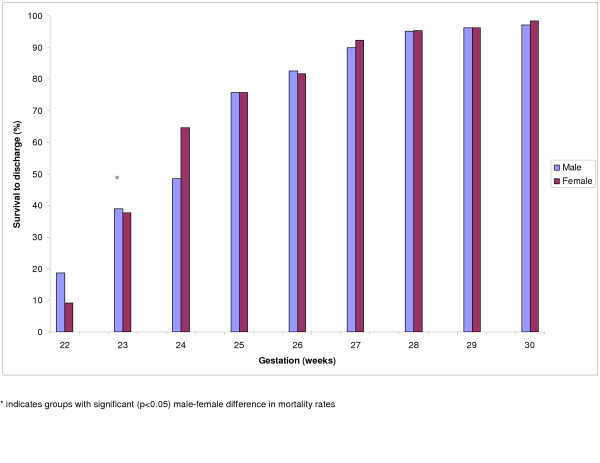
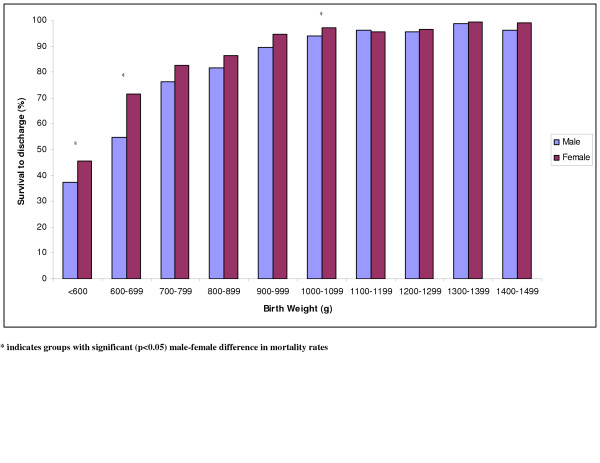
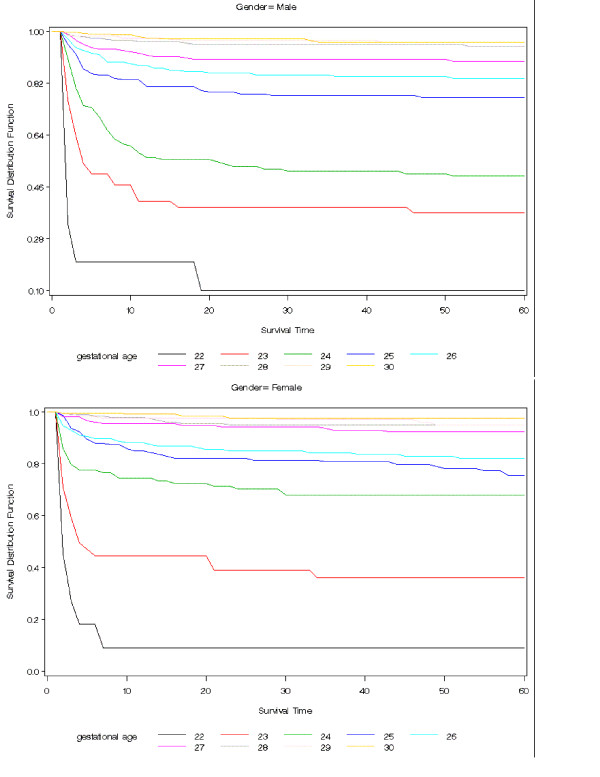
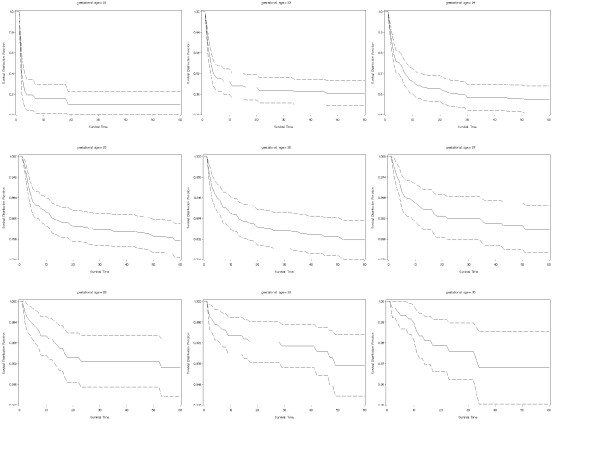
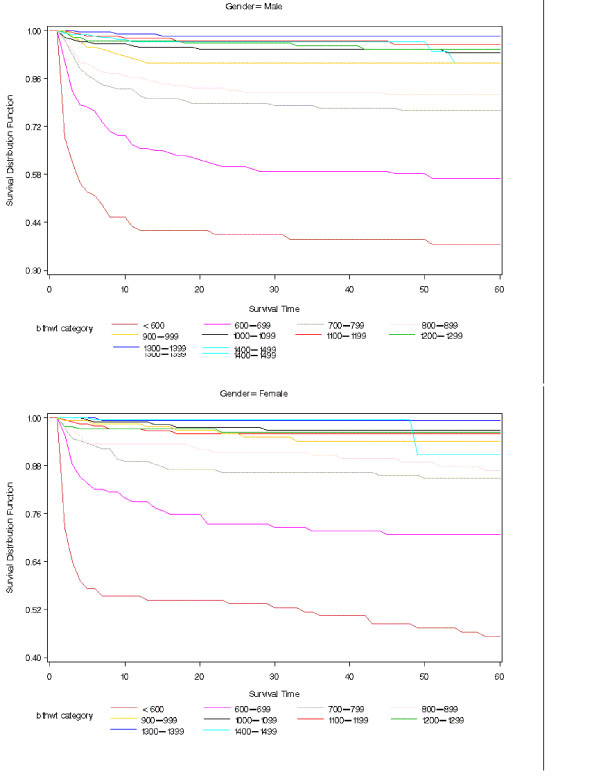
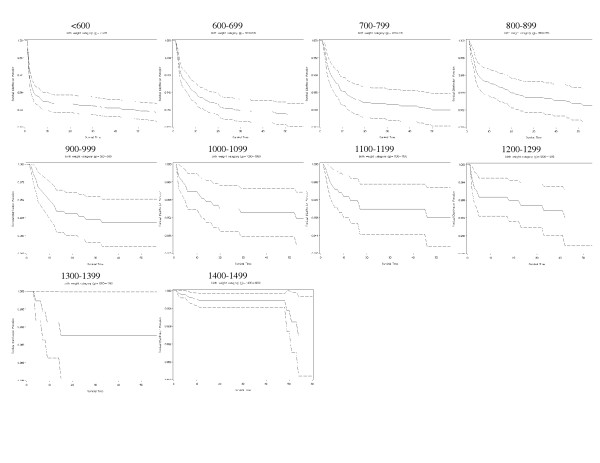
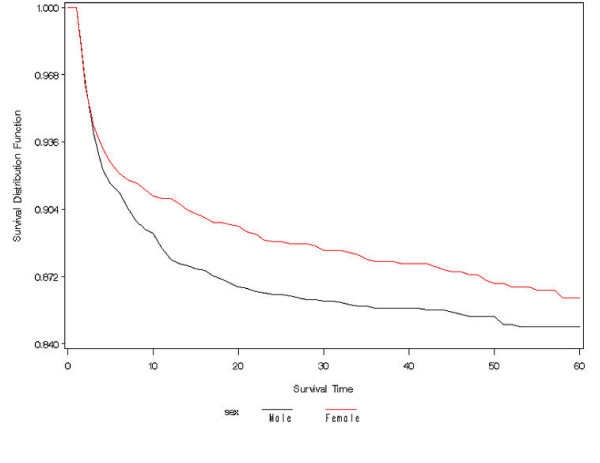
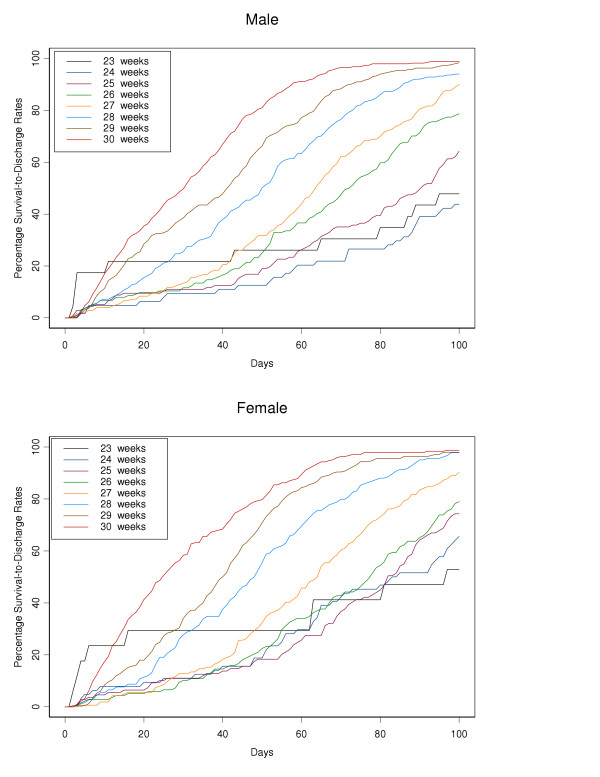
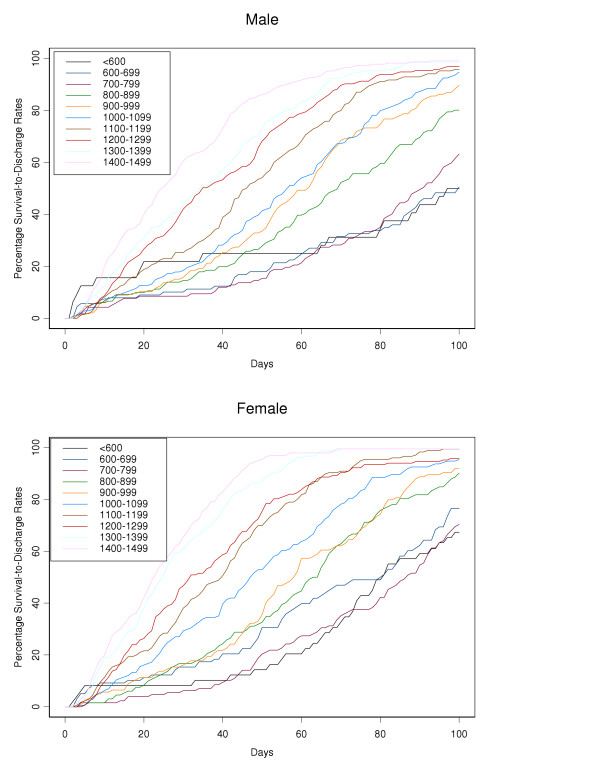
Results: Survival to discharge at 24 weeks gestation was 54%, compared to 82% at 26 weeks and 95% at 30 weeks. In infants with birth weights 600-699, survival to discharge was 62%, compared to 79% at 700-799 g and 96% at 1,000-1,099 g. In infants born at 24 weeks gestational age, survival was higher in females but there were no significant gender differences above 24 weeks gestation. Actuarial analysis showed that risk of death was highest in the first 5 days. For infants born at 24 weeks gestation, estimated survival probability to 48 hours, 7 days and 4 weeks were 88 (CI 84, 92)%, 70 (CI 64, 76)% and 60 (CI 53, 66)% respectively. For smaller birth weights, female survival probabilities were higher than males for the first 40 days of life.
Conclusion: Actuarial analysis provides useful information when counseling parents and highlights the importance of frequently revising the prediction for long term survival particularly after the first few days of life.
Figures
References
-
- Hack M, Wright LL, Shankaran S, Tyson JE, Horbar JD, Bauer CR, Younes N. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Network, November 1989 to October 1990. Am J Obstet Gynecol. 1995;172:457–464. doi: 10.1016/0002-9378(95)90557-X. - DOI - PubMed
-
- Fanaroff AA, Wright LL, Stevenson DK, Shankaran S, Donovan EP, Ehrenkranz RA, Younes N, Korones SB, Stoll BJ, Tyson JE, Bauer CR, Oh W, Lemons JA, Papile LA, Verter J. Very low birthweight outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, May 1991 through December 1992. Am J Obstet Gynecol. 1995;173:1423–1431. doi: 10.1016/0002-9378(95)90628-2. - DOI - PubMed
-
- Stevenson DK, Wright LL, Lemons JA, Oh W, Korones SB, Papile LA, Bauer CR, Stoll BJ, Tyson JE, Shankaran S, Fanaroff AA, Donovan EF, Ehrenkranz RA, Verter J. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, January 1993 through December 1994. Am J Obstet Gynecol. 1998;179:1632–1639. doi: 10.1016/S0002-9378(98)70037-7. - DOI - PubMed
-
- Ferrara TB, Hoekstra RE, Couser RJ, Gaziano EP, Calvin SE, Payne NR, Fangman JJ. Survival and follow-up of infants born at 23–26 weeks of gestational age: effects of surfactant therapy. J Pediatr. 1994;124:119–124. - PubMed
-
- Jobe AH, Mitchell BR, Gunkel JH. Beneficial effects of the combined use of prenatal corticosteroids and postnatal surfactant on preterm infants. Am J Obstet Gynecol. 1993;168:508–513. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
