

Solitary fibrous tumor in the thigh: review of the literature
- PMID: 16283380
- PMCID: PMC12161049
- DOI: 10.1007/s00432-005-0055-7
Solitary fibrous tumor in the thigh: review of the literature
Abstract
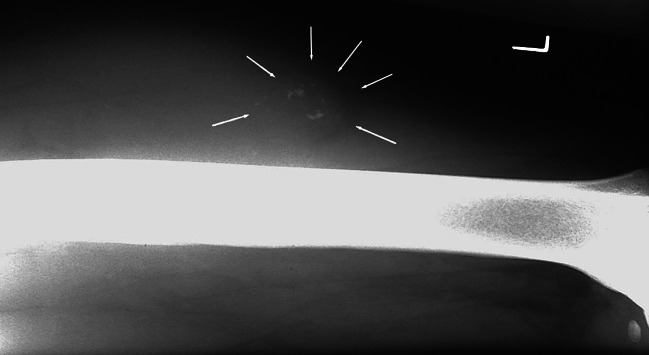
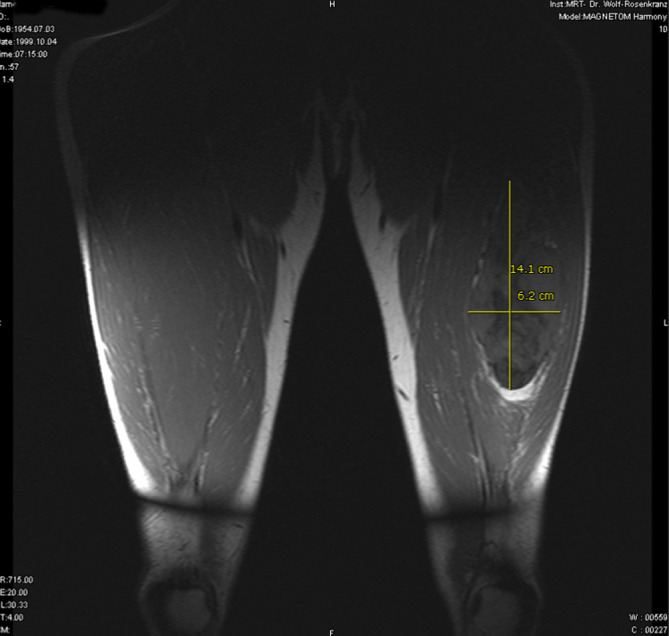
Solitary fibrous tumors (SFT) of extremities, especially the thighs are very rare. Despite SFTs are generally benign, well-circumscribed soft tissue tumors new cases should be presented and followed up carefully to monitor their biological behavior. In general for tumor classification a biopsy is state of the art. Histological including immunohistochemical patterns for SFTs are defined. MRI and ultrasound are not sufficient for differential diagnosis. Once property identified and defined by size and location, resection with intact tumor capsule may result in full recovery of the patient. Reviewing the literature there are no validated reasons for a wider resection. The current patient was a 41-year-old male. Four years after an arthroscopy of the left knee the patient has been suffering an ongoing swelling of the lateral thigh. Because MRI scan data suggested a synovial sarcoma a biopsy was performed. The tumor was classified as a benign SFT. The diagnosis based on histological findings and the presence of the positive immunohistochemical markers Vimentin, CD34, and CD99. The complete tumor resection with intact capsule was achieved in a final operation. Clinical and in MRI after 54-month outcome period there were no local recurrences.
Figures



Similar articles
-
What Are the Complications, Function, and Survival of Tumor-devitalized Autografts Used in Patients With Limb-sparing Surgery for Bone and Soft Tissue Tumors? A Japanese Musculoskeletal Oncology Group Multi-institutional Study.Clin Orthop Relat Res. 2023 Nov 1;481(11):2110-2124. doi: 10.1097/CORR.0000000000002720. Epub 2023 Jun 14. Clin Orthop Relat Res. 2023. PMID: 37314384 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Contrast-enhanced ultrasound using SonoVue® (sulphur hexafluoride microbubbles) compared with contrast-enhanced computed tomography and contrast-enhanced magnetic resonance imaging for the characterisation of focal liver lesions and detection of liver metastases: a systematic review and cost-effectiveness analysis.Health Technol Assess. 2013 Apr;17(16):1-243. doi: 10.3310/hta17160. Health Technol Assess. 2013. PMID: 23611316 Free PMC article.
-
What Are the Recurrence Rates, Complications, and Functional Outcomes After Multiportal Arthroscopic Synovectomy for Patients With Knee Diffuse-type Tenosynovial Giant-cell Tumors?Clin Orthop Relat Res. 2024 Jul 1;482(7):1218-1229. doi: 10.1097/CORR.0000000000002934. Epub 2023 Dec 28. Clin Orthop Relat Res. 2024. PMID: 38153106 Free PMC article.
Cited by
-
A locally aggressive solitary fibrous tumor of the leg: Case report and literature review.Int J Surg Case Rep. 2012;3(5):177-80. doi: 10.1016/j.ijscr.2012.01.009. Epub 2012 Feb 11. Int J Surg Case Rep. 2012. PMID: 22387414 Free PMC article.
-
Indeterminate soft-tissue tumors of the hand and wrist: a review based on a clinical series of 39 cases.Skeletal Radiol. 2011 Aug;40(8):977-89. doi: 10.1007/s00256-010-1009-y. Epub 2010 Jul 31. Skeletal Radiol. 2011. PMID: 20680624 Review.
-
Extrapleural solitary fibrous tumor evidenced by 68Ga-prostate-specific membrane antigen positron emission tomography/computed tomography study in the staging of a high-risk prostate cancer patient.World J Nucl Med. 2020 Jul 22;19(4):425-427. doi: 10.4103/wjnm.WJNM_18_20. eCollection 2020 Oct-Dec. World J Nucl Med. 2020. PMID: 33623515 Free PMC article.
-
Solitary fibrous tumour of gluteus: a case report about an uncommon localization of a rare neoplasm.J Surg Case Rep. 2016 Jun 22;2016(6):rjw111. doi: 10.1093/jscr/rjw111. J Surg Case Rep. 2016. PMID: 27333919 Free PMC article.
-
Soft tissue solitary fibrous tumor. Imaging findings in a series of nine cases.Skeletal Radiol. 2012 Nov;41(11):1427-33. doi: 10.1007/s00256-012-1364-y. Epub 2012 Feb 16. Skeletal Radiol. 2012. PMID: 22349595
References
-
- Abe S, Imamura T, Tateishi A, Park P, Nakano H, Harasawa A, Hashimoto H, Matsushita T (1999) Intramuscular solitary fibrous tumor: a clinicopathological case study. J Comp Assist Tomo 23(3):458–462 - PubMed
-
- Ahn J, Shim J, Yang W, Kim T (2001) Meningeal solitary fibrous tumor as an unusual cause of expohthalmos: case report and review of the literature. Neurosurgery 48(6):1362–1366 - PubMed
-
- Akisue T, Matsumoto K, Kizaki T, Fujita I, Yamamoto T, Yoshiya S, Kurosaka M (2003) Solitary fibrous tumor in the extremity: case report and review of the literature. Clin Orthop 411:236–244 - PubMed
-
- Akiyama Y, Nabeshima K, Koita H, Yamanaka M, Koono M (2000) Solitary fibrous tumor of the vagina. Pathol Int 50(4):327–331 - PubMed
-
- Alexander M, Yang S, Yung R, Brasic J, Pannu H (2004) Diagnosis of benign solitary fibrous tumors by positron emission tomography. South Med J 97(12):1264–1267 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
