

Radiologic morphology of low-grade primary central nervous system lymphoma in immunocompetent patients
- PMID: 16286384
- PMCID: PMC7976218
Radiologic morphology of low-grade primary central nervous system lymphoma in immunocompetent patients
Abstract
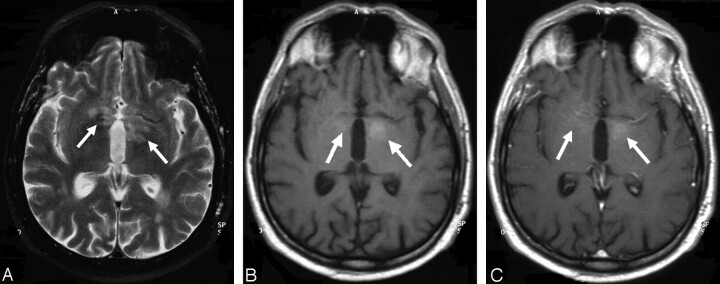
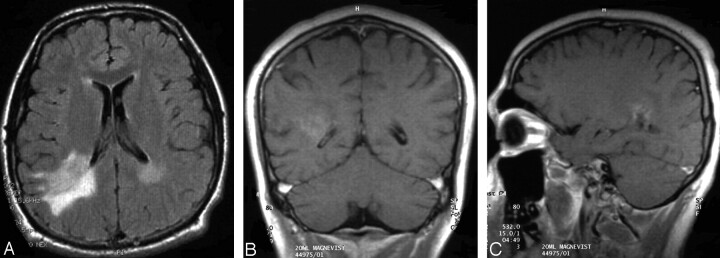
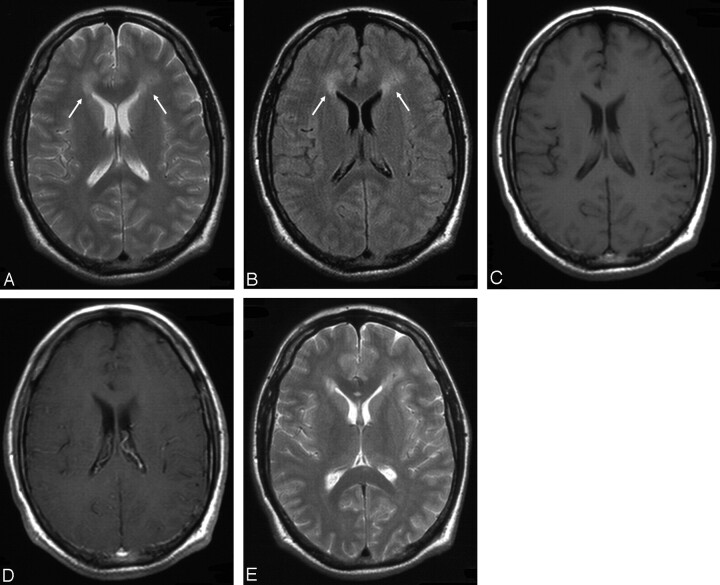
Background and purpose: Primary central nervous system lymphomas (PCNSLs) are usually high-grade and are rarely low-grade non-Hodgkin lymphomas (NHLs). On MR imaging, PCNSLs typically present as contrast-enhancing lesions in contact with the subarachnoid space without evidence of necrosis. We evaluated the radiologic morphology and clinical characteristics of low-grade PCNSLs, hypothesizing that they may differ from high-grade PCNSLs.
Methods: Records were reviewed from 332 patients screened for inclusion in 3 multicenter prospective trials. MR imaging scans were obtained from all patients and were centrally reviewed by 2 consultant neuroradiologists.
Results: Ten patients (3%) with low-grade PCNSLs (7 men and 3 women; median age, 59 years; age range, 19-61 years) were identified. Four patients had one lesion, 2 patients 2 lesions, and 4 patients had multiple lesions. The following radiologic features infrequently seen in high-grade PCNSLs were found in a substantial proportion of patients: location in deep structures or spine (n = 6); lack of periventricular location (n = 5); hyperintensity on T2-weighted images (n = 10); moderate or absent contrast enhancement (n = 6); and heterogeneous contrast enhancement (n = 5). In 8 patients, >2 of these features were present in at least one lesion, and, thus, the radiologic appearance was assessed atypical of high-grade PCNSLs. The atypical radiologic appearance in combination with atypical or mild symptoms resulted in a false or delayed diagnosis.
Conclusion: Low-grade PCNSLs may have a variable and atypical radiologic morphology compared with high-grade PCNSLs with the risk of false or delayed diagnosis.
Figures



Similar articles
-
Utility of dynamic contrast-enhanced magnetic resonance imaging for differentiating glioblastoma, primary central nervous system lymphoma and brain metastatic tumor.Eur J Radiol. 2016 Oct;85(10):1722-1727. doi: 10.1016/j.ejrad.2016.07.005. Epub 2016 Jul 15. Eur J Radiol. 2016. PMID: 27666608
-
Differentiation of primary central nervous system lymphoma and high-grade glioma with dynamic susceptibility contrast-enhanced perfusion magnetic resonance imaging.Acta Radiol. 2009 Mar;50(2):217-25. doi: 10.1080/02841850802616752. Acta Radiol. 2009. PMID: 19096950
-
Diffusion kurtosis imaging differs between primary central nervous system lymphoma and high-grade glioma and is correlated with the diverse nuclear-to-cytoplasmic ratio: a histopathologic, biopsy-based study.Eur Radiol. 2020 Apr;30(4):2125-2137. doi: 10.1007/s00330-019-06544-7. Epub 2019 Dec 19. Eur Radiol. 2020. PMID: 31858206
-
[New developments in diagnosis and therapy of primary non-Hodgkin's lymphoma of the central nervous system].Nervenarzt. 1997 Apr;68(4):298-308. doi: 10.1007/s001150050128. Nervenarzt. 1997. PMID: 9273459 Review. German.
-
Primary central nervous system lymphoma.Arch Pathol Lab Med. 2008 Nov;132(11):1830-4. doi: 10.5858/132.11.1830. Arch Pathol Lab Med. 2008. PMID: 18976024 Review.
Cited by
-
Case report. Primary hypothalamic third ventriclular Burkitt's lymphoma: a case report with emphasis on differential diagnosis.Br J Radiol. 2010 Feb;83(986):e43-7. doi: 10.1259/bjr/84426981. Br J Radiol. 2010. PMID: 20139257 Free PMC article.
-
Primary solitary retro-clival amyloidoma.Surg Neurol Int. 2018 May 15;9:100. doi: 10.4103/sni.sni_483_17. eCollection 2018. Surg Neurol Int. 2018. PMID: 29900030 Free PMC article.
-
Dural masses: meningiomas and their mimics.Insights Imaging. 2019 Feb 6;10(1):11. doi: 10.1186/s13244-019-0697-7. Insights Imaging. 2019. PMID: 30725238 Free PMC article. Review.
-
Neuroimaging of acute and chronic unilateral and bilateral thalamic lesions.Insights Imaging. 2019 Feb 22;10(1):24. doi: 10.1186/s13244-019-0700-3. Insights Imaging. 2019. PMID: 30796553 Free PMC article. Review.
-
Utility of proton MR spectroscopy for differentiating typical and atypical primary central nervous system lymphomas from tumefactive demyelinating lesions.AJNR Am J Neuroradiol. 2014 Feb;35(2):270-7. doi: 10.3174/ajnr.A3677. Epub 2013 Aug 8. AJNR Am J Neuroradiol. 2014. PMID: 23928144 Free PMC article.
References
-
- Plasswilm L, Herrlinger U, Korfel A, et al. Primary central nervous system (CNS) lymphoma in immunocompetent patients. Ann Hematol 2002;81:415–423 - PubMed
-
- Fine HA, Mayer RJ. Primary central nervous system lymphoma. Ann Intern Med 1993;119:1093–1104 - PubMed
-
- Eby NL, Gruffermann S, Flannelly CM, et al. Increasing incidence of primary brain lymphoma in the US. Cancer 1988;62:2461–2465 - PubMed
-
- Herrlinger U, Schabet M, Brugger W, et al. German Cancer Society Neuro-Oncology Working Group NOA-03 multicenter trial of single-agent high-dose methotrexate for primary central nervous system lymphoma. Ann Neurol 2002;51:247–252 - PubMed
-
- Jahnke K, Korfel A, Martus P, et al. High-dose methotrexate toxicity in elderly patients with primary central nervous system lymphoma. Ann Oncol 2005;16:445–449 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources