

Preliminary experience with Leo self-expanding stent for the treatment of intracranial aneurysms
Affiliations
- PMID: 16286403
- PMCID: PMC7976185
Item in Clipboard
Preliminary experience with Leo self-expanding stent for the treatment of intracranial aneurysms
AJNR Am J Neuroradiol.
2005 Nov-Dec.
Abstract
We report initial experience with the use of a new intracranial stent, the Leo microstent in combination with detachable coils in treatment of patients with wide-necked cerebral aneurysms. The Leo stent represents a significant advance in the vascular treatment of intracranial aneurysm with high radial force and an easy delivery system. It is a feasible, secure, and effective system.
Figures
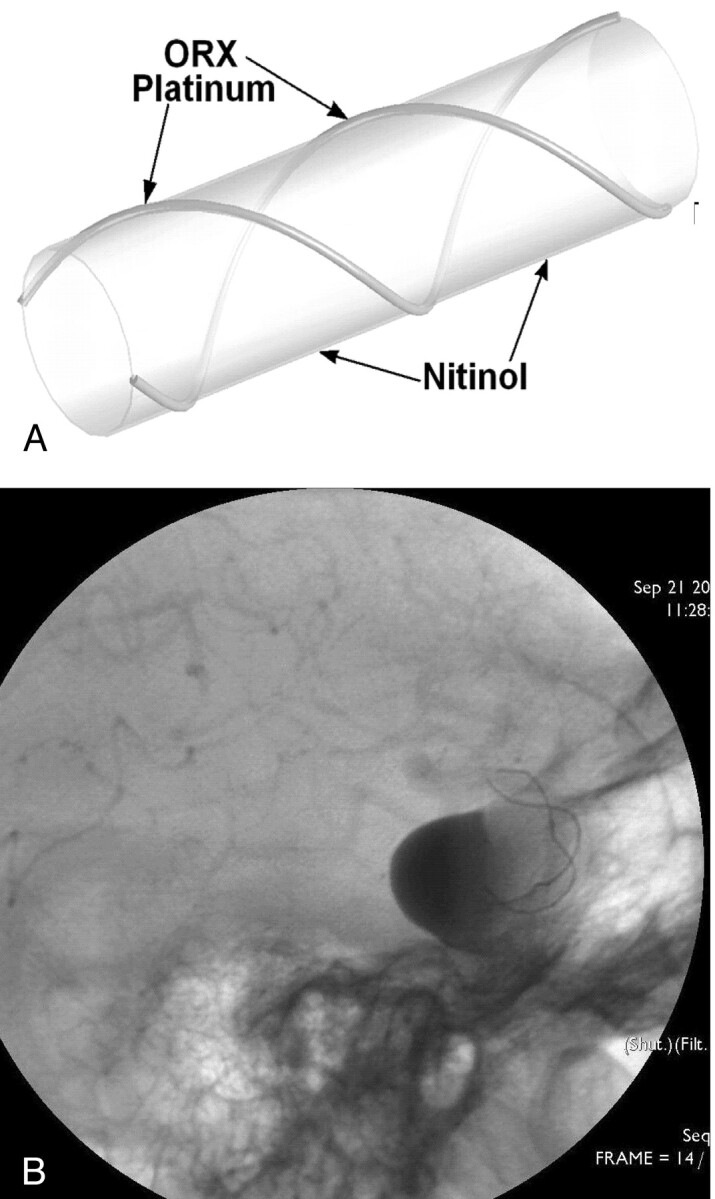
A, A twisted nitinol wire body and 2 platinum markers. B, ORX visualization of both diameter and length.
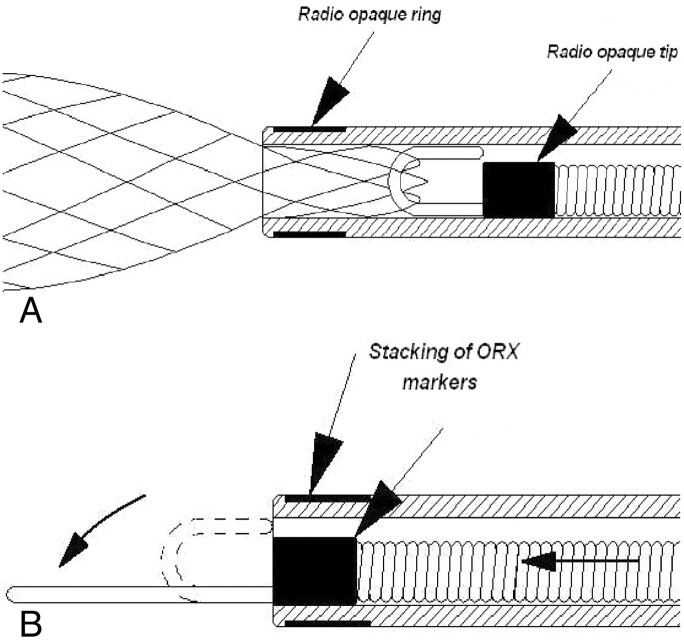
A and B, The innovative Leo stent distal hook.
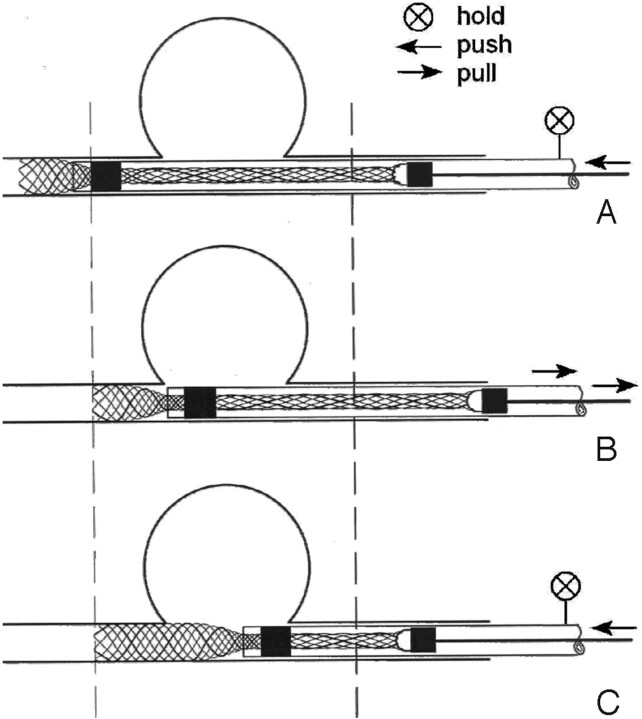
A, Depressing the pusher to make the stent extend approximately 5 mm. B, Pulling the catheter and the stent back until the distal end of the stent is precisely positioned. C, Once the distal end of the stent is positioned, it may be delivered by depressing the pusher. The catheter is self-retrieving.
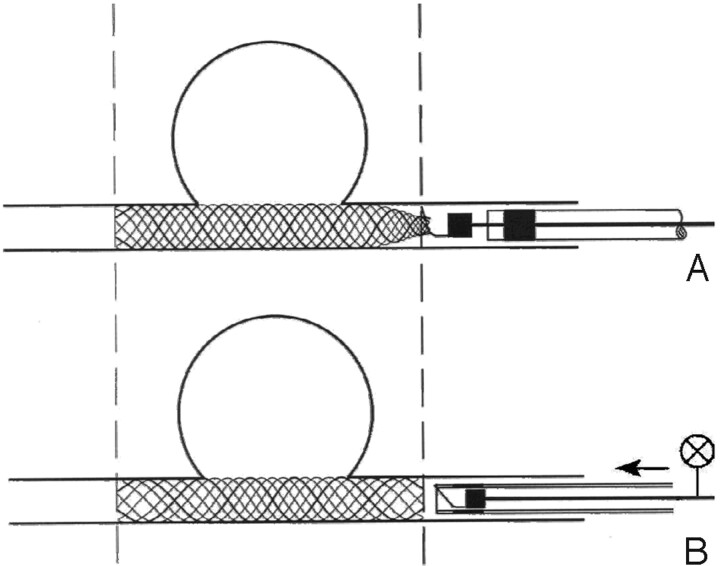
A, When the pusher comes out of the Vasco catheter (staking of ORX markers), the stent is fully out and cannot be resheathed, but it is still attached to the hook. B, To detach the stent, it is then necessary to resheath the pusher inside the catheter by advancing the catheter.
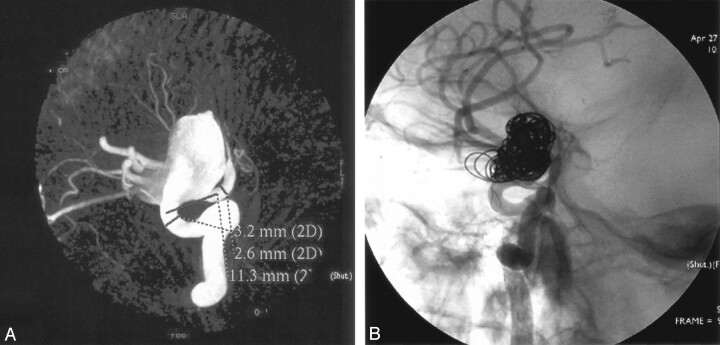
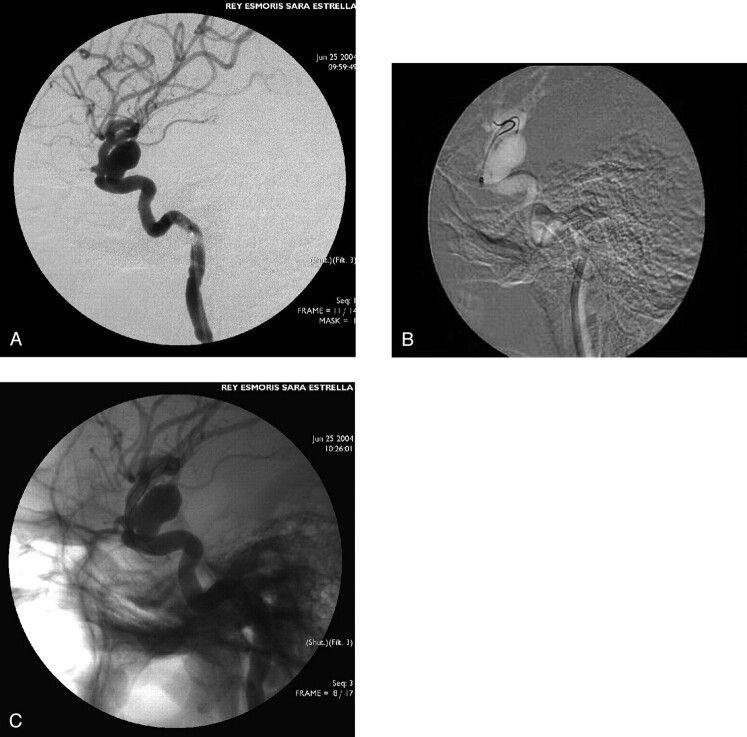
A, Reconstructed image from a 3D rotational angiogram demonstrating a wide-necked paraophthalmic aneurysm of the cavernous internal carotid artery. B, Angiogram obtained after stent deployment and after coiling through the stent interstices shows aneurysm is occluded.
A, Prowler microcatheter in place within a cavernous aneurysm through the interstices of the stent. B, Coiling of aneurysm across the stent. C, Finally, total exclusion of the aneurysm.
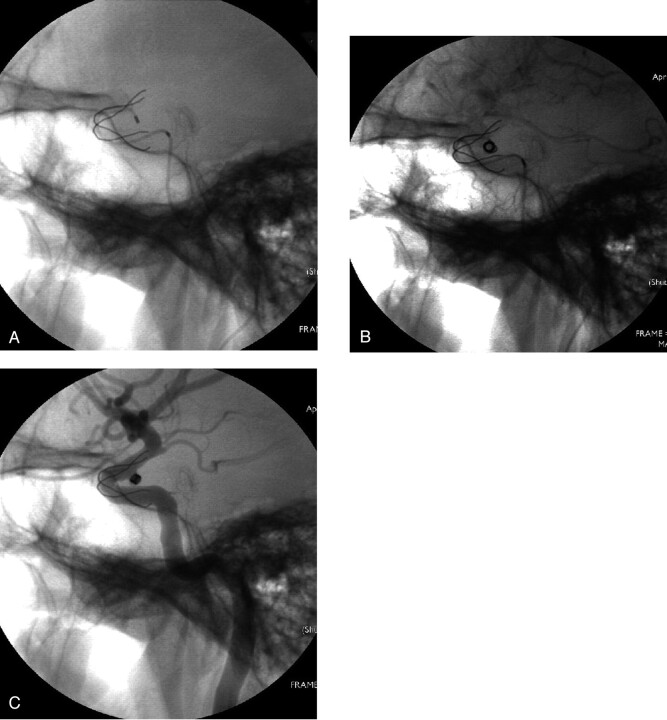
A, Aneurysm of the cavernous internal carotid artery. B, Two microwires (.0014 inches), which make advancing the Leo stent easier. C, An implanted Leo stent.
References
-
- Howington JU, Hanel RA, Harrigan MR, et al. The Neuroform stent, the first microcatheter-delivered stent for use in the intracranial circulation. Neurosurgery 2004;54:2–5 - PubMed
-
- Fiorella D, Albuquerque FC, Han P, et al. Preliminary experience using the Neuroform stent for the treatment of cerebral aneurysms. Neurosurgery 2004;54:6–17 - PubMed
-
- Benitez RP, Silva MT, Klem J, et al. Endovascular occlusion of wide-necked aneurysms with a new intracranial microstent (Neuroform) and detachable coils. Neurosurgery 2004;54:1359–1368 - PubMed
-
- Sani S, Jobe KW, and Lopes DK. Treatment of wide-necked cerebral aneurysms with the Neuroform2 Treo stent. Neurosurg Focus 2005;4:1–5 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical