

Maternal-fetal microtransfusions and HIV-1 mother-to-child transmission in Malawi
- PMID: 16287342
- PMCID: PMC1285069
- DOI: 10.1371/journal.pmed.0030010
Maternal-fetal microtransfusions and HIV-1 mother-to-child transmission in Malawi
Abstract
Background: Between 25% and 35% of infants born to HIV-infected mothers become HIV-1 infected. One potential route of mother-to-child transmission (MTCT) could be through a breakdown in the placental barrier (i.e., maternal-fetal microtransfusions).
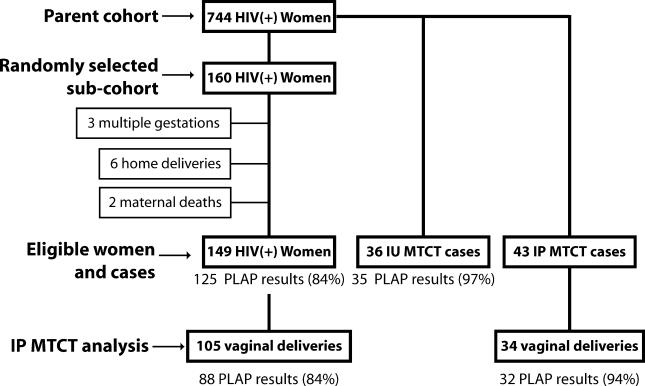
Methods and findings: Placental alkaline phosphatase (PLAP) is a 130-kD maternal enzyme that cannot cross the intact placental barrier. We measured PLAP activity in umbilical vein serum as an indicator of maternal-fetal microtransfusion, and related this to the risk of HIV-1 MTCT. A case-cohort study was conducted of 149 women randomly selected from a cohort of HIV-1-infected pregnant Malawians; these women served as a reference group for 36 cases of in utero MTCT and 43 cases of intrapartum (IP) MTCT. Cord PLAP activity was measured with an immunocatalytic assay. Infant HIV status was determined by real-time PCR. The association between cord PLAP activity and HIV-1 MTCT was measured with logistic regression using generalized estimating equations. Among vaginal deliveries, PLAP was associated with IP MTCT (risk ratio, 2.25 per log10 ng/ml PLAP; 95% confidence interval, 0.95-5.32) but not in utero MTCT. In a multivariable model adjusted for HIV-1 RNA load, chorioamnionitis, and self-reported fever, the risk of IP MTCT almost tripled for every log10 increase in cord PLAP activity (risk ratio, 2.87; 95% confidence interval, 1.05-7.83).
Conclusion: These results suggest that during vaginal deliveries, placental microtransfusions are a risk factor for IP HIV-1 MTCT. Future studies are needed to identify factors that increase the risk for microtransfusions in order to prevent IP HIV-1 MTCT.
Conflict of interest statement
References
-
- Joint United Nations Programme on HIV/AIDS, World Health Organization. Joint United Nations Programme on HIV/AIDS, World Health Organization (2004) AIDS epidemic update: December 2004. 2004 Available: http://www.unaids.org/wad2004/EPI_1204_pdf_en/EpiUpdate04_en.pdf. Accessed 12 October 2005.
-
- De Cock KM, Fowler MG, Mercier E, de Vincenzi I, Saba J, et al. Prevention of mother-to-child HIV transmission in resource-poor countries: Translating research into policy and practice. JAMA. 2000;283:1175–1182. - PubMed
-
- Kourtis AP, Bulterys M, Nesheim SR, Lee FK. Understanding the timing of HIV transmission from mother to infant. JAMA. 2001;285:709–712. - PubMed
-
- Van de Perre P. Mother-to-child transmission of HIV-1: the ‘all mucosal' hypothesis as a predominant mechanism of transmission. AIDS. 1999;13:1133–1138. - PubMed
-
- European Mode of Delivery Collaboration. Elective caesarean-section versus vaginal delivery in prevention of vertical HIV-1 transmission: A randomised clinical trial. Lancet. 1999;353:1035–1039. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
