

Carbohydrate restriction improves the features of Metabolic Syndrome. Metabolic Syndrome may be defined by the response to carbohydrate restriction
- PMID: 16288655
- PMCID: PMC1323303
- DOI: 10.1186/1743-7075-2-31
Carbohydrate restriction improves the features of Metabolic Syndrome. Metabolic Syndrome may be defined by the response to carbohydrate restriction
Abstract
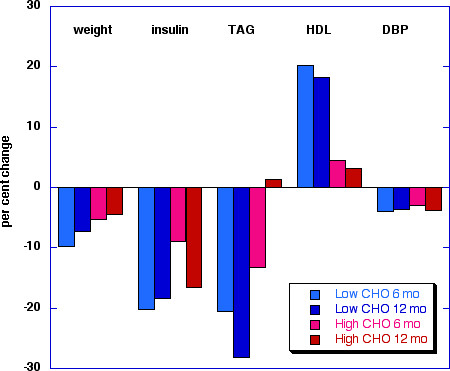
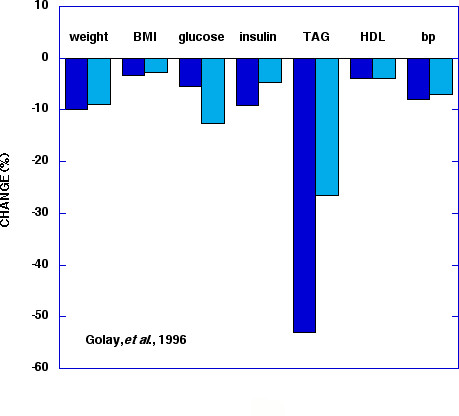
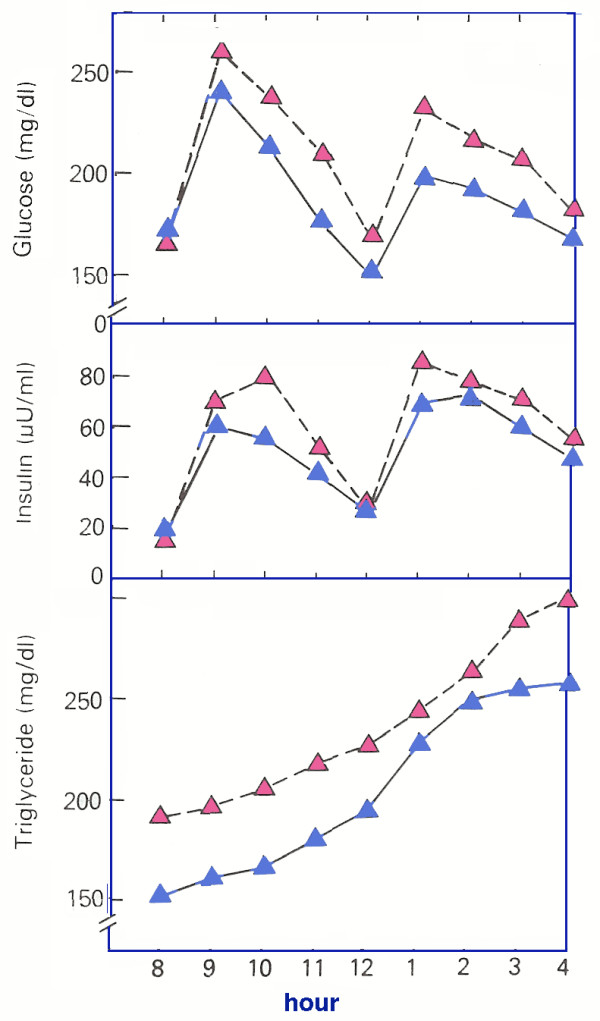
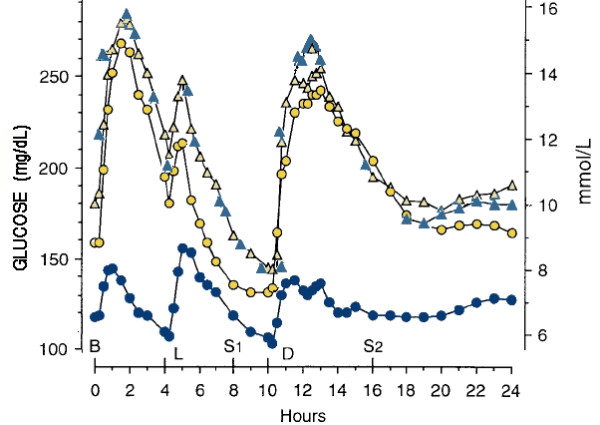
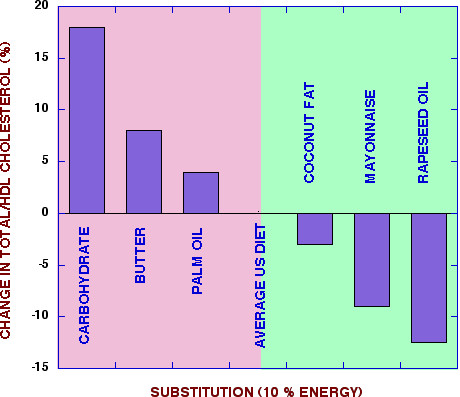
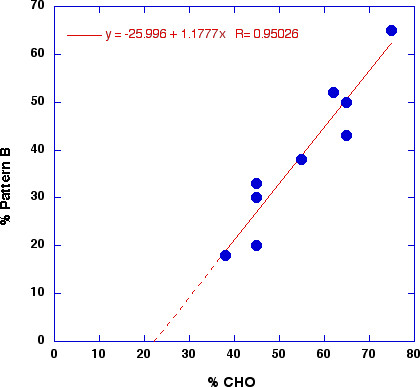
Metabolic Syndrome (MetS) represents a constellation of markers that indicates a predisposition to diabetes, cardiovascular disease and other pathologic states. The definition and treatment are a matter of current debate and there is not general agreement on a precise definition or, to some extent, whether the designation provides more information than the individual components. We consider here five indicators that are central to most definitions and we provide evidence from the literature that these are precisely the symptoms that respond to reduction in dietary carbohydrate (CHO). Carbohydrate restriction is one of several strategies for reducing body mass but even in the absence of weight loss or in comparison with low fat alternatives, CHO restriction is effective at ameliorating high fasting glucose and insulin, high plasma triglycerides (TAG), low HDL and high blood pressure. In addition, low fat, high CHO diets have long been known to raise TAG, lower HDL and, in the absence of weight loss, may worsen glycemic control. Thus, whereas there are numerous strategies for weight loss, a patient with high BMI and high TAG is likely to benefit most from a regimen that reduces CHO intake. Reviewing the literature, benefits of CHO restriction are seen in normal or overweight individuals, in normal patients who meet the criteria for MetS or in patients with frank diabetes. Moreover, in low fat studies that ameliorate LDL and total cholesterol, controls may do better on the symptoms of MetS. On this basis, we feel that MetS is a meaningful, useful phenomenon and may, in fact, be operationally defined as the set of markers that responds to CHO restriction. Insofar as this is an accurate characterization it is likely the result of the effect of dietary CHO on insulin metabolism. Glucose is the major insulin secretagogue and insulin resistance has been tied to the hyperinsulinemic state or the effect of such a state on lipid metabolism. The conclusion is probably not surprising but has not been explicitly stated before. The known effects of CHO-induced hypertriglyceridemia, the HDL-lowering effect of low fat, high CHO interventions and the obvious improvement in glucose and insulin from CHO restriction should have made this evident. In addition, recent studies suggest that a subset of MetS, the ratio of TAG/HDL, is a good marker for insulin resistance and risk of CVD, and this indicator is reliably reduced by CHO restriction and exacerbated by high CHO intake. Inability to make this connection in the past has probably been due to the fact that individual responses have been studied in isolation as well as to the emphasis of traditional therapeutic approaches on low fat rather than low CHO. We emphasize that MetS is not a disease but a collection of markers. Individual physicians must decide whether high LDL, or other risk factors are more important than the features of MetS in any individual case but if MetS is to be considered it should be recognized that reducing CHO will bring improvement. Response of symptoms to CHO restriction might thus provide a new experimental criterion for MetS in the face of on-going controversy about a useful definition. As a guide to future research, the idea that control of insulin metabolism by CHO intake is, to a first approximation, the underlying mechanism in MetS is a testable hypothesis.
Figures
References
-
- Grundy SM, Brewer HBJ, Cleeman JI, Smith SCJ, Lenfant C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation. 2004;109(3):433–438. doi: 10.1161/01.CIR.0000111245.75752.C6. - DOI - PubMed
-
- Grundy SM, Hansen B, Smith SCJ, Cleeman JI, Kahn RA. Clinical management of metabolic syndrome: report of the American Heart Association/National Heart, Lung, and Blood Institute/American Diabetes Association conference on scientific issues related to management. Arterioscler Thromb Vasc Biol. 2004;24(2):e19–24. doi: 10.1161/01.ATV.0000112379.88385.67. - DOI - PubMed
-
- Tonkin A. The metabolic syndrome -- a growing problem. European Heart Journal Supplements. 2004;6:A37–A42.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
