

The anatomy of decision support during inpatient care provider order entry (CPOE): empirical observations from a decade of CPOE experience at Vanderbilt
- PMID: 16290243
- PMCID: PMC1518541
- DOI: 10.1016/j.jbi.2005.08.009
The anatomy of decision support during inpatient care provider order entry (CPOE): empirical observations from a decade of CPOE experience at Vanderbilt
Abstract
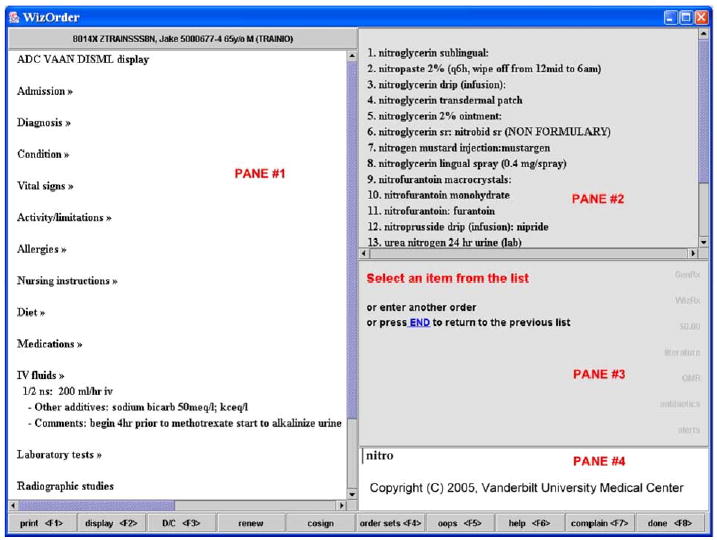
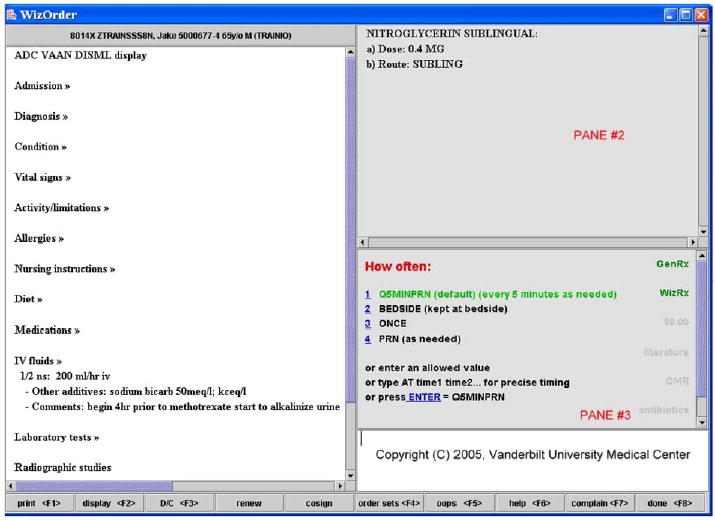
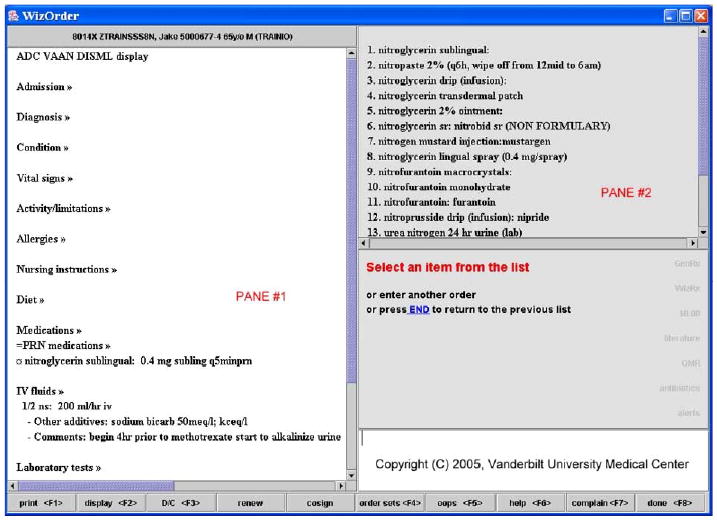
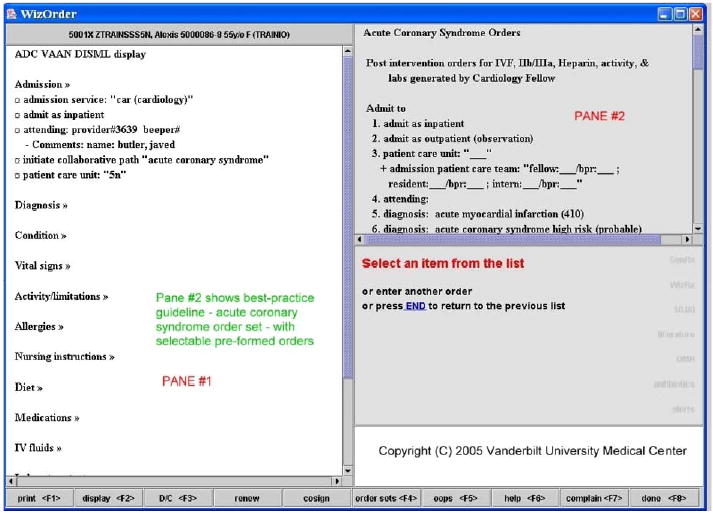
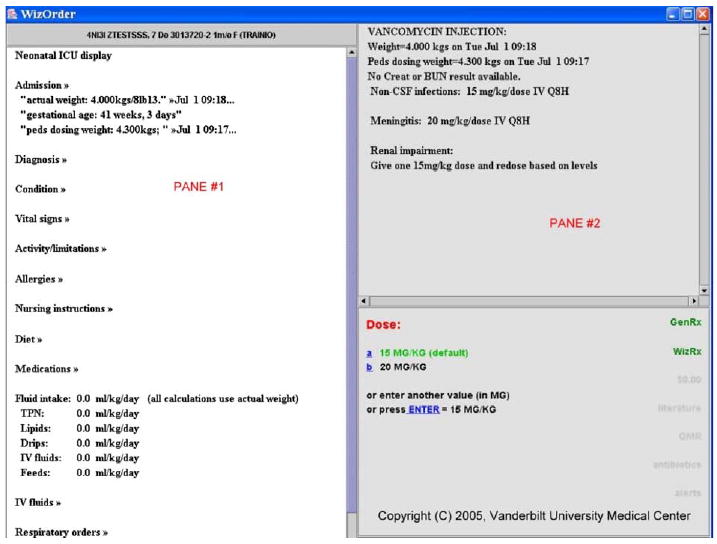
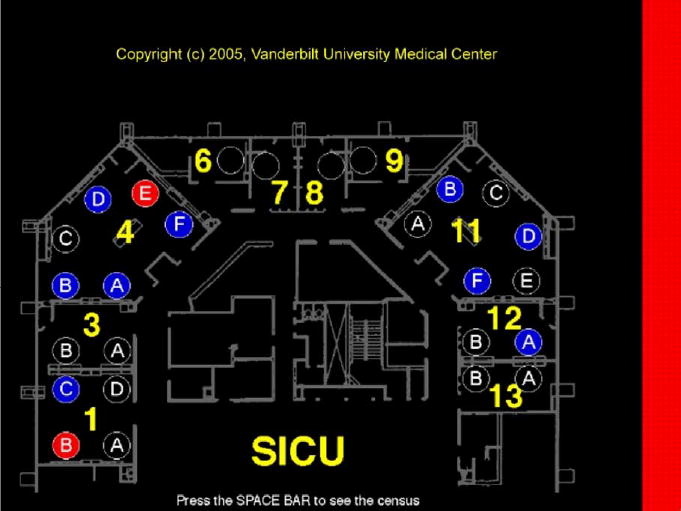
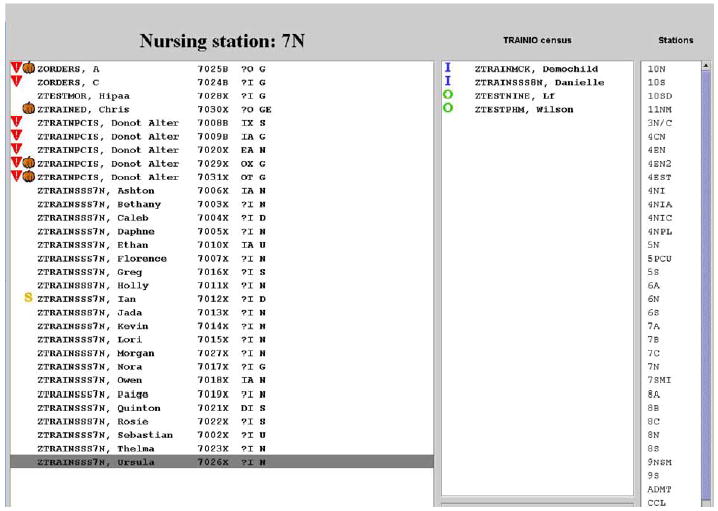
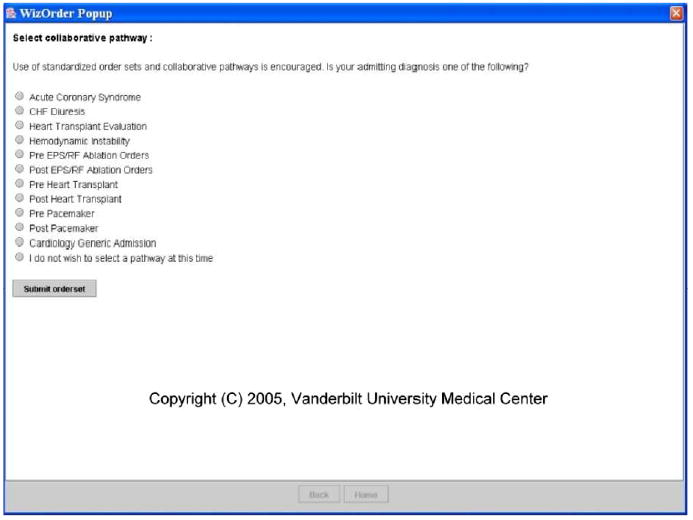
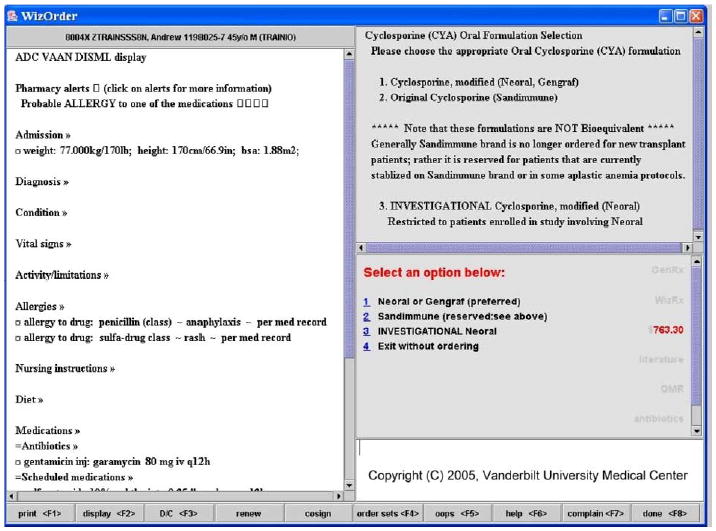
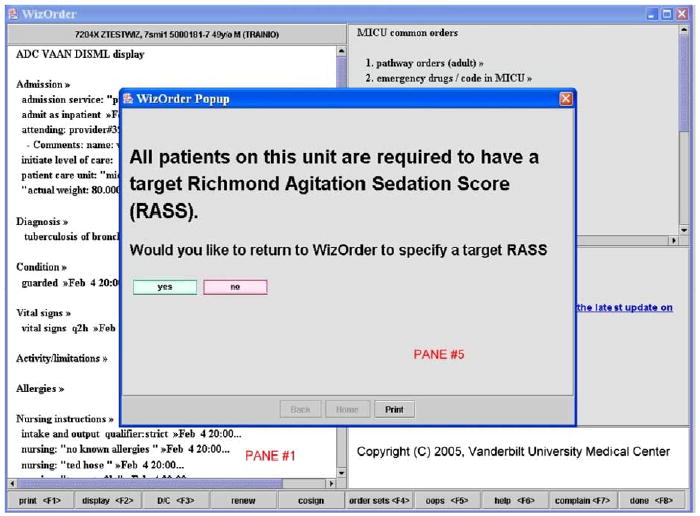
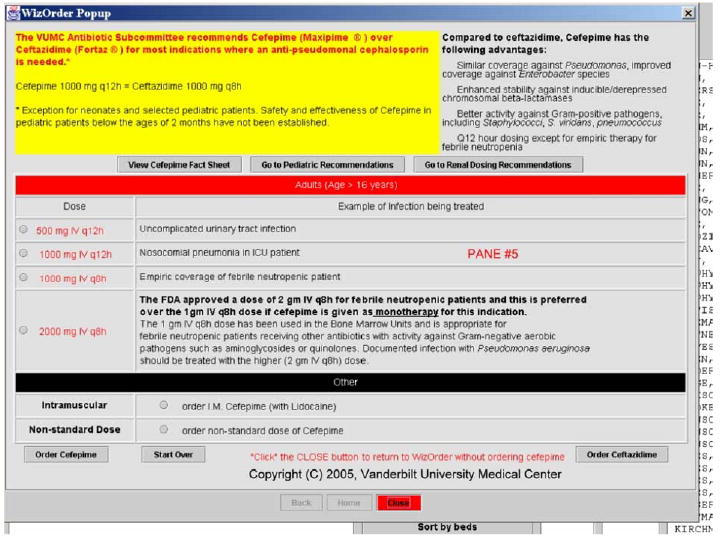
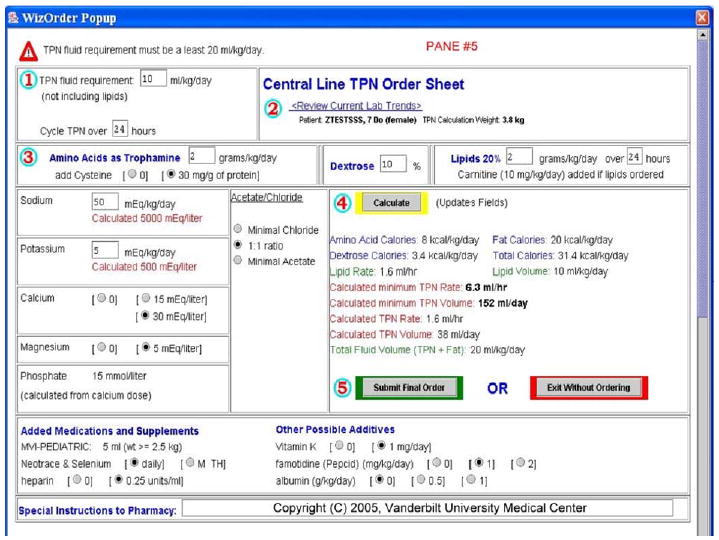
The authors describe a pragmatic approach to the introduction of clinical decision support at the point of care, based on a decade of experience in developing and evolving Vanderbilt's inpatient "WizOrder" care provider order entry (CPOE) system. The inpatient care setting provides a unique opportunity to interject CPOE-based decision support features that restructure clinical workflows, deliver focused relevant educational materials, and influence how care is delivered to patients. From their empirical observations, the authors have developed a generic model for decision support within inpatient CPOE systems. They believe that the model's utility extends beyond Vanderbilt, because it is based on characteristics of end-user workflows and on decision support considerations that are common to a variety of inpatient settings and CPOE systems. The specific approach to implementing a given clinical decision support feature within a CPOE system should involve evaluation along three axes: what type of intervention to create (for which the authors describe 4 general categories); when to introduce the intervention into the user's workflow (for which the authors present 7 categories), and how disruptive, during use of the system, the intervention might be to end-users' workflows (for which the authors describe 6 categories). Framing decision support in this manner may help both developers and clinical end-users plan future alterations to their systems when needs for new decision support features arise.
Figures

References
-
- Kassirer JP, Gorry GA. Clinical problem solving: a behavioral analysis. Ann Intern Med. 1978;89(2):245–55. - PubMed
-
- Covell DG, Uman GC, Manning PR. Information needs in office practice: are they being met? Ann Intern Med. 1985;103(4):596–599. - PubMed
-
- Kassirer JP, Kopelman RI. Knowledge and clinical expertise. Hosp Pract (Off Ed) 1988;23(3):46. 53, 57 passim. - PubMed
-
- Jelovsek FR, Rittwage J, Pearse WH, Visscher HC. Information management needs of the obstetrician-gynecologist—a survey. Obstet Gynecol. 1989;73(3 Pt 1):395–9. - PubMed
-
- Williamson JW, German PS, Weiss R, Skinner EA, Bowes third F. Health science information management and continuing education of physicians. A survey of U.S. primary care practitioners and their opinion leaders. Ann Intern Med. 1989;110(2):151–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
