

Efficacy of intensive multitherapy for patients with type 2 diabetes mellitus: a randomized controlled trial
- PMID: 16293781
- PMCID: PMC1316161
- DOI: 10.1503/cmaj.050054
Efficacy of intensive multitherapy for patients with type 2 diabetes mellitus: a randomized controlled trial
Abstract
Background: National guidelines for managing diabetes set standards for care. We sought to determine whether a 1-year intensive multitherapy program resulted in greater goal attainment than usual care among patients with poorly controlled type 2 diabetes mellitus.
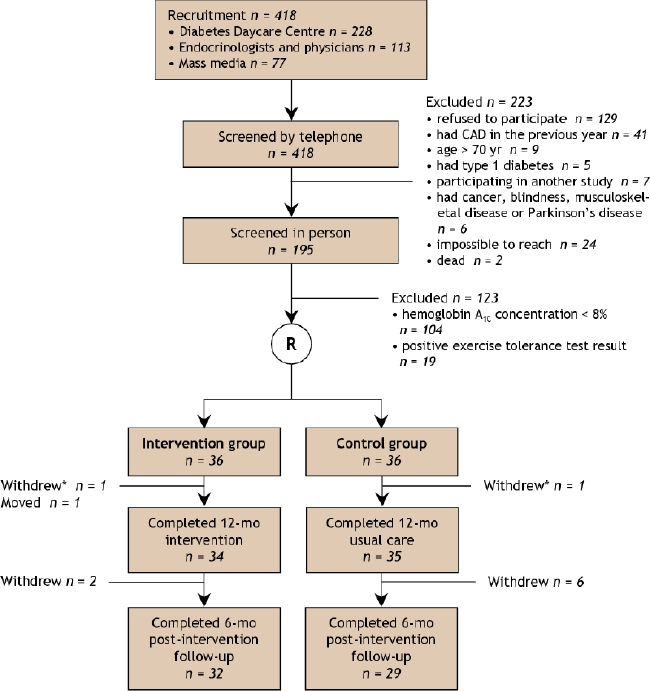
Methods: We identified patients with poorly controlled type 2 diabetes receiving outpatient care in the community or at our hospital. Patients 30-70 years of age with a hemoglobin A1c concentration of 8% or greater were randomly assigned to receive intensive multitherapy (n = 36) or usual care (n = 36).
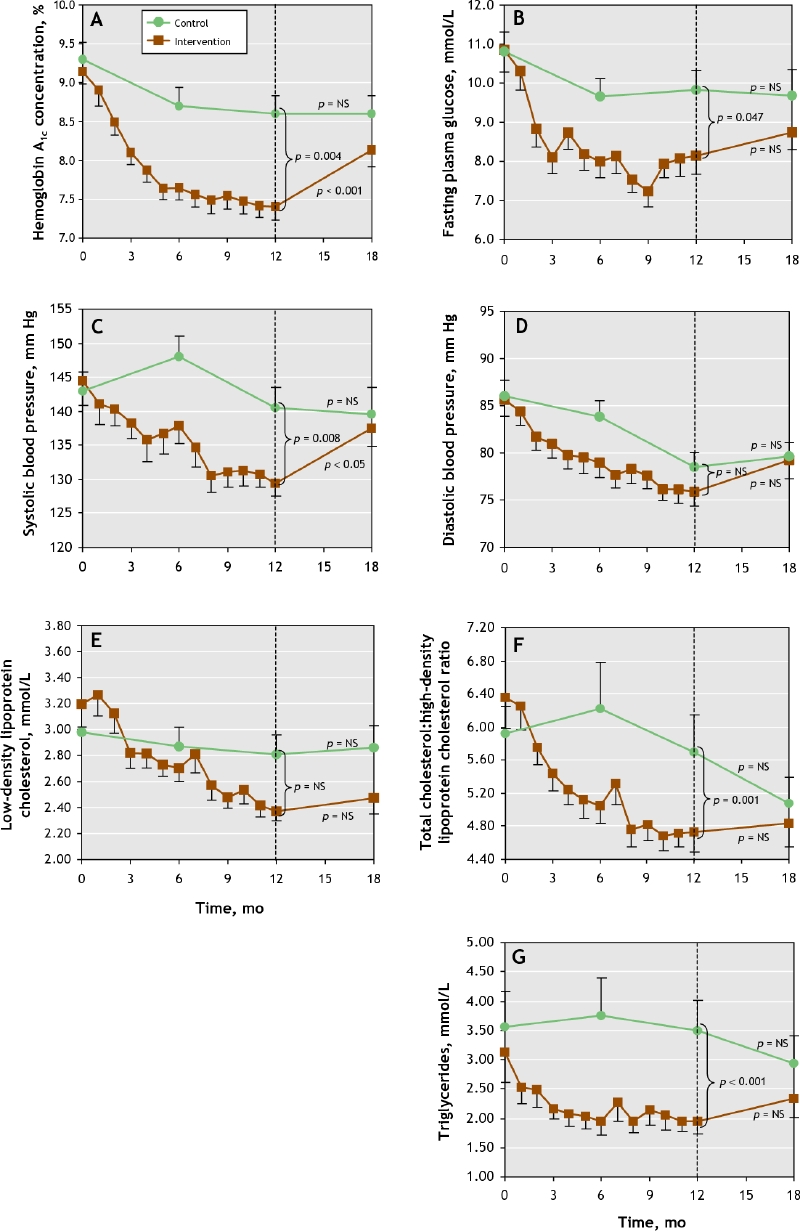
Results: The average hemoglobin A1c concentration at entry was 9.1% (standard deviation [SD] 1%) in the intensive therapy group and 9.3% (SD 1%) in the usual therapy group. By 12 months, a higher proportion of patients in the intensive therapy group than in the control group had achieved Canadian Diabetes Association (CDA) goals for hemoglobin A(1c) concentrations (goal < or = 7.0%: 35% v. 8%), diastolic blood pressure (goal < 80 mm Hg: 64% v. 37%), low-density lipoprotein cholesterol (LDL-C) levels (goal < 2.5 mmol/L: 53% v. 20%) and triglyceride levels (goal < 1.5 mmol/L: 44% v. 14%). There were no significant differences between the 2 groups in attaining the targets for fasting plasma glucose levels, systolic blood pressure or total cholesterol:high-density lipoprotein cholesterol ratio. None of the patients reached all CDA treatment goals. By 18 months, differences in goal attainment were no longer evident between the 2 groups, except for LDL-C levels. Quality of life, as measured by a specific questionnaire, increased in both groups, with a greater increase in the intensive therapy group (13% [SD 10%] v. 6% [SD 13%], p < 0.003).
Interpretation: Intensive multitherapy for patients with poorly controlled type 2 diabetes is successful in helping patients meet most of the goals set by a national diabetes association. However, 6 months after intensive therapy stopped and patients returned to usual care, the benefits had vanished.
Figures
Comment in
-
Can diabetes management programs create sustained improvements in disease outcomes?CMAJ. 2005 Dec 6;173(12):1467-8. doi: 10.1503/cmaj.051343. CMAJ. 2005. PMID: 16330635 Free PMC article. No abstract available.
-
Multitherapy for diabetes.CMAJ. 2006 Nov 7;175(10):1246-7; author reply 1247. doi: 10.1503/cmaj.1060019. CMAJ. 2006. PMID: 17098957 Free PMC article. No abstract available.
-
Multitherapy for diabetes.CMAJ. 2006 Nov 7;175(10):1247-8. doi: 10.1503/cmaj.1060002. CMAJ. 2006. PMID: 17098959 Free PMC article. No abstract available.
References
-
- UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes: UKPDS 33. Lancet 1998;352:837-53. - PubMed
-
- Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Lancet 2000;355(9200):253-9. Erratum in: Lancet 2000;356(9232):860. - PubMed