

Interaction of ritonavir-boosted tipranavir with loperamide does not result in loperamide-associated neurologic side effects in healthy volunteers
- PMID: 16304151
- PMCID: PMC1315935
- DOI: 10.1128/AAC.49.12.4903-4910.2005
Interaction of ritonavir-boosted tipranavir with loperamide does not result in loperamide-associated neurologic side effects in healthy volunteers
Abstract
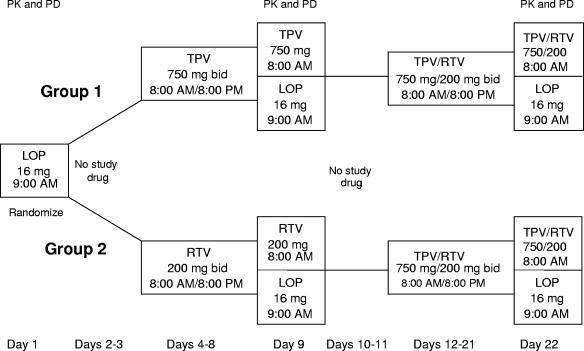
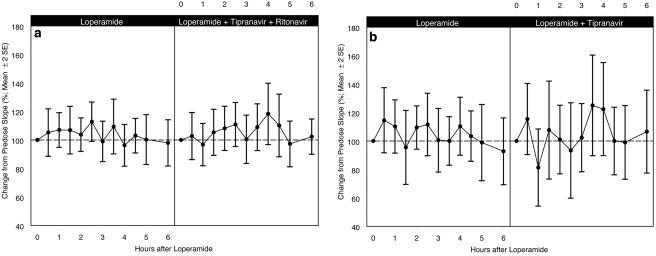
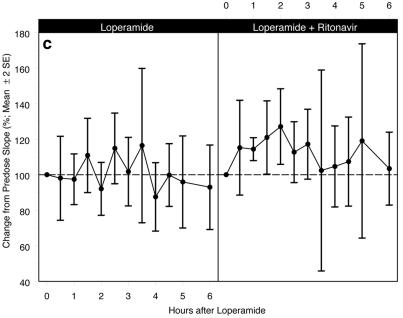
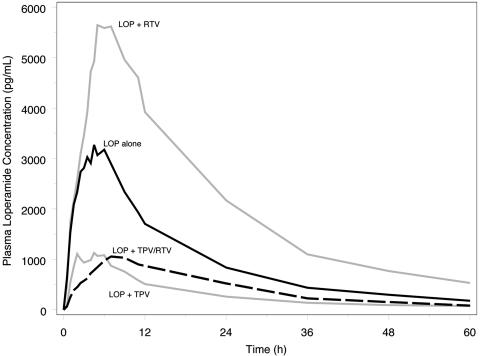
Loperamide (LOP) is a peripherally acting opioid receptor agonist used for the management of chronic diarrhea through the reduction of gut motility. The lack of central opioid effects is partly due to the efflux activity of the multidrug resistance transporter P-glycoprotein (P-gp) at the blood-brain barrier. The protease inhibitors are substrates for P-gp and have the potential to cause increased LOP levels in the brain. Because protease inhibitors, including tipranavir (TPV), are often associated with diarrhea, they are commonly used in combination with LOP. The level of respiratory depression, the level of pupil constriction, the pharmacokinetics, and the safety of LOP alone compared with those of LOP-ritonavir (RTV), LOP-TPV, and LOP-TPV-RTV were evaluated in a randomized, open-label, parallel-group study with 24 healthy human immunodeficiency virus type 1-negative adults. Respiratory depression was assessed by determination of the ventilatory response to carbon dioxide. Tipranavir-containing regimens (LOP-TPV and LOP-TPV-RTV) caused decreases in the area under the concentration-time curve from time zero to infinity for LOP (51% and 63% decreases, respectively) and its metabolite (72% and 77% decreases, respectively), whereas RTV caused increases in the levels of exposure of LOP (121% increase) and its metabolite (44% increase). In vitro and in vivo data suggest that TPV is a substrate for and an inducer of P-gp activity. The respiratory response to LOP in combination with TPV and/or RTV was not different from that to LOP alone. There was no evidence that LOP had opioid effects in the central nervous system, as measured indirectly by CO2 response curves and pupillary response in the presence of TPV and/or RTV.
Figures
References
-
- Back, N. K., A. van Wijk, D. Remmerswaal, M. van Monfort, M. Nijhuis, R. Schuurman, and C. A. Boucher. 2000. In-vitro tipranavir susceptibility of HIV-1 isolates with reduced susceptibility of other protease inhibitors. AIDS 14:101-102. - PubMed
-
- Drewe, J., H. Gutmann, G. Fricker, M. Torok, C. Belinger, and J. Huwyler. 1999. HIV protease inhibitor ritonavir: a more potent inhibitor of P-glycoprotein than the cyclosporine analog SDZ PSC 833. Biochem. Pharmacol. 57:1147-1152. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
