

Effective antimicrobial regimens for use in humans for therapy of Bacillus anthracis infections and postexposure prophylaxis
- PMID: 16304178
- PMCID: PMC1315931
- DOI: 10.1128/AAC.49.12.5099-5106.2005
Effective antimicrobial regimens for use in humans for therapy of Bacillus anthracis infections and postexposure prophylaxis
Abstract
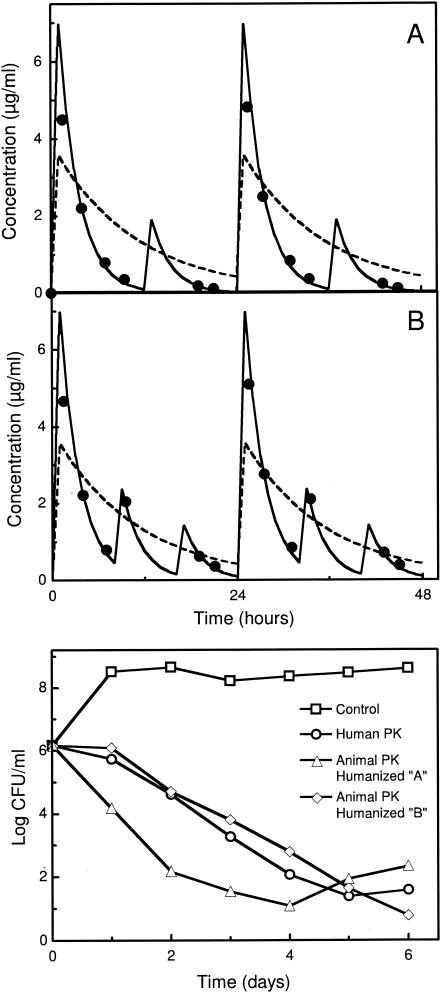
Expanded options for treatments directed against pathogens that can be used for bioterrorism are urgently needed. Treatment regimens directed against such pathogens can be identified only by using data derived from in vitro and animal studies. It is crucial that these studies reliably predict the efficacy of proposed treatments in humans. The objective of this study was to identify a levofloxacin treatment regimen that will serve as an effective therapy for Bacillus anthracis infections and postexposure prophylaxis. An in vitro hollow-fiber infection model that replicates the pharmacokinetic profile of levofloxacin observed in humans (half-life [t(1/2)], 7.5 h) or in animals, such as the mouse or the rhesus monkey (t(1/2), approximately 2 h), was used to evaluate a proposed indication for levofloxacin (500 mg once daily) for the treatment of Bacillus anthracis infections. The results obtained with the in vitro model served as the basis for the doses and the dose schedules that were evaluated in the mouse inhalational anthrax model. The effects of levofloxacin and ciprofloxacin treatment were compared to those of no treatment (untreated controls). The main outcome measure in the in vitro hollow-fiber infection model was a persistent reduction of culture density (> or = 4 log10 reduction) and prevention of the emergence of levofloxacin-resistant organisms. In the mouse inhalational anthrax model the main outcome measure was survival. The results indicated that levofloxacin given once daily with simulated human pharmacokinetics effectively sterilized Bacillus anthracis cultures. By using a simulated animal pharmacokinetic profile, a once-daily dosing regimen that provided a human-equivalent exposure failed to sterilize the cultures. Dosing regimens that "partially humanized" levofloxacin exposures within the constraints of animal pharmacokinetics reproduced the antimicrobial efficacy seen with human pharmacokinetics. In a mouse inhalational anthrax model, once-daily dosing was significantly inferior (survival end point) to regimens of dosing every 12 h or every 6 h with identical total daily levofloxacin doses. These results demonstrate the predictive value of the in vitro hollow-fiber infection model with respect to the success or the failure of treatment regimens in animals. Furthermore, the model permits the evaluation of treatment regimens that "humanize" antibiotic exposures in animal models, enhancing the confidence with which animal models may be used to reliably predict the efficacies of proposed antibiotic treatments in humans in situations (e.g., the release of pathogens as agents of bioterrorism or emerging infectious diseases) where human trials cannot be performed. A treatment regimen effective in rhesus monkeys was identified.
Figures




Similar articles
-
Pharmacokinetic considerations and efficacy of levofloxacin in an inhalational anthrax (postexposure) rhesus monkey model.Antimicrob Agents Chemother. 2006 Nov;50(11):3535-42. doi: 10.1128/AAC.00090-06. Antimicrob Agents Chemother. 2006. PMID: 17065619 Free PMC article.
-
Postexposure Prophylaxis and Treatment of Bacillus anthracis Infections: A Systematic Review and Meta-analyses of Animal Models, 1947-2019.Clin Infect Dis. 2022 Oct 17;75(Suppl 3):S379-S391. doi: 10.1093/cid/ciac591. Clin Infect Dis. 2022. PMID: 36251546 Free PMC article.
-
Pharmacokinetic-pharmacodynamic analysis of fluoroquinolones against Bacillus anthracis.J Infect Chemother. 2004 Apr;10(2):97-100. doi: 10.1007/s10156-004-0303-9. J Infect Chemother. 2004. PMID: 15160302
-
Obiltoxaximab Prevents Disseminated Bacillus anthracis Infection and Improves Survival during Pre- and Postexposure Prophylaxis in Animal Models of Inhalational Anthrax.Antimicrob Agents Chemother. 2016 Sep 23;60(10):5796-805. doi: 10.1128/AAC.01102-16. Print 2016 Oct. Antimicrob Agents Chemother. 2016. PMID: 27431219 Free PMC article.
-
Management of anthrax meningitis.Lancet Infect Dis. 2005 May;5(5):287-95. doi: 10.1016/S1473-3099(05)70113-4. Lancet Infect Dis. 2005. PMID: 15854884 Review.
Cited by
-
Aerosolized Bacillus anthracis infection in New Zealand white rabbits: natural history and intravenous levofloxacin treatment.Comp Med. 2010 Dec;60(6):461-8. Comp Med. 2010. PMID: 21262133 Free PMC article.
-
Marmosets as models of infectious diseases.Front Cell Infect Microbiol. 2024 Feb 23;14:1340017. doi: 10.3389/fcimb.2024.1340017. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38465237 Free PMC article. Review.
-
Use of an in vitro pharmacodynamic model to derive a linezolid regimen that optimizes bacterial kill and prevents emergence of resistance in Bacillus anthracis.Antimicrob Agents Chemother. 2008 Jul;52(7):2486-96. doi: 10.1128/AAC.01439-07. Epub 2008 May 5. Antimicrob Agents Chemother. 2008. PMID: 18458134 Free PMC article.
-
Pharmacokinetics-pharmacodynamics of pyrazinamide in a novel in vitro model of tuberculosis for sterilizing effect: a paradigm for faster assessment of new antituberculosis drugs.Antimicrob Agents Chemother. 2009 Aug;53(8):3197-204. doi: 10.1128/AAC.01681-08. Epub 2009 May 18. Antimicrob Agents Chemother. 2009. PMID: 19451303 Free PMC article.
-
Efficacy of oritavancin in a murine model of Bacillus anthracis spore inhalation anthrax.Antimicrob Agents Chemother. 2008 Sep;52(9):3350-7. doi: 10.1128/AAC.00360-08. Epub 2008 Jul 7. Antimicrob Agents Chemother. 2008. PMID: 18606841 Free PMC article.
References
-
- Atlas, R. M. 2002. Bioterriorism: from threat to reality. Annu. Rev. Microbiol. 56:167-185. - PubMed
-
- Bilello, J. A., G. Bauer, M. N. Dudley, G. A. Cole, and G. L. Drusano. 1994. The effect of 2′,3′-didehydro-3′-deoxythymidine (D4T) in an in vitro hollow fiber pharmacodynamic model system correlates with results of dose- ranging clinical studies. Antimicrob. Agents Chemother. 38:1386-1391. - PMC - PubMed
-
- Bilello, J. A., P. A. Bilello, J. J. Kort, M. N. Dudley, J. Leonard, and G. L. Drusano. 1995. Efficacy of constant infusion of A-77003, an inhibitor of the human immunodeficiency virus (HIV) protease in limiting acute HIV type 1 infection in vitro. Antimicrob. Agents Chemother. 39:2523-2527. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
