

Origin of ICU acquired paresis determined by direct muscle stimulation
- PMID: 16306155
- PMCID: PMC2077517
- DOI: 10.1136/jnnp.2005.070813
Origin of ICU acquired paresis determined by direct muscle stimulation
Abstract
Background: Acquired diffuse paresis in an intensive care unit (ICU) can result from critical illness myopathy or polyneuropathy. Clinical examination and conventional neurophysiological techniques may not distinguish between these entities.
Objective: To assess the value of direct muscle stimulation (DMS) to differentiate myopathic from neuropathic process in critically ill patients with diffuse severe muscle weakness.
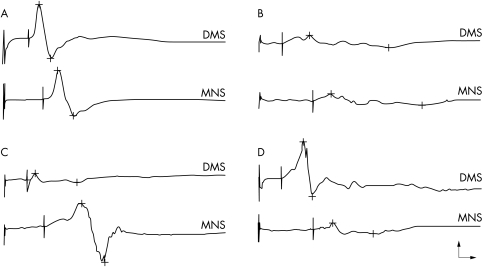
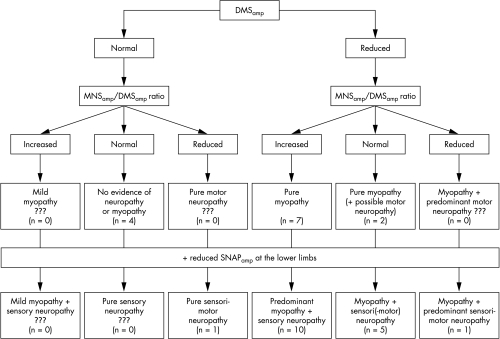
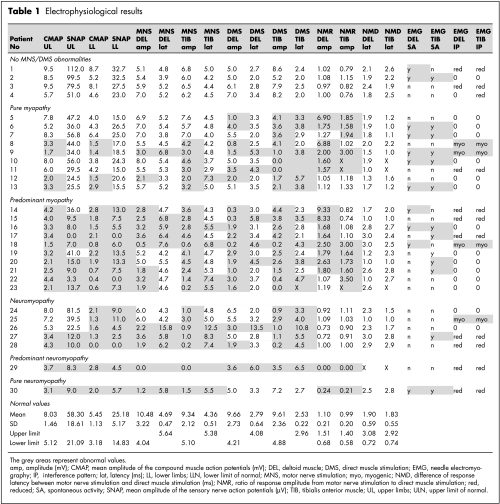
Methods: 30 consecutive patients with ICU acquired diffuse motor weakness were studied. Responses of the right deltoid and tibialis anterior muscles to DMS and to motor nerve stimulation (MNS) were studied and compared with results of conventional nerve conduction studies and concentric needle electromyography (EMG). An original algorithm was used for differential diagnosis, taking into account first the amplitude of the responses to DMS, then the MNS to DMS amplitude ratio, and finally the amplitude of the sensory nerve action potentials recorded at the lower limbs.
Results: Evidence of neuropathy and myopathy was found in 57% and 83% of the patients, respectively. Pure or predominant myopathy was found in 19 patients. Other results were consistent with neuromyopathy (n = 5) and pure or predominant neuropathy (n = 2). Four patients had normal results with stimulation techniques, but spontaneous EMG activity and raised plasma creatine kinase suggesting necrotic myopathy.
Conclusions: A neurophysiological approach combining DMS and conventional techniques revealed myopathic processes in a majority of ICU patients. Reduced muscle fibre excitability may be a leading cause for this. The diagnosis of myopathy in ICU acquired paralysis can be established by a combination of DMS, needle EMG, and plasma creatine kinase.
Conflict of interest statement
Competing interests: none declared
References
-
- Bolton C F. Neuromuscular conditions in the intensive care unit. Intensive Care Med 199622841–843. - PubMed
-
- Lacomis D, Giuliani M J, Van Cott A.et al Acute myopathy of intensive care: clinical, electromyographic, and pathological aspects. Ann Neurol 199640645–654. - PubMed
-
- Latronico N, Fenzi F, Recupero D.et al Critical illness myopathy and neuropathy. Lancet 19963471579–1582. - PubMed
-
- McFarlane L A, Rosenthal F D. Severe myopathy after status asthmaticus. Lancet 1977ii615 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical