

Design of the VA/NIH Acute Renal Failure Trial Network (ATN) Study: intensive versus conventional renal support in acute renal failure
- PMID: 16317811
- PMCID: PMC1351394
- DOI: 10.1191/1740774505cn116oa
Design of the VA/NIH Acute Renal Failure Trial Network (ATN) Study: intensive versus conventional renal support in acute renal failure
Abstract
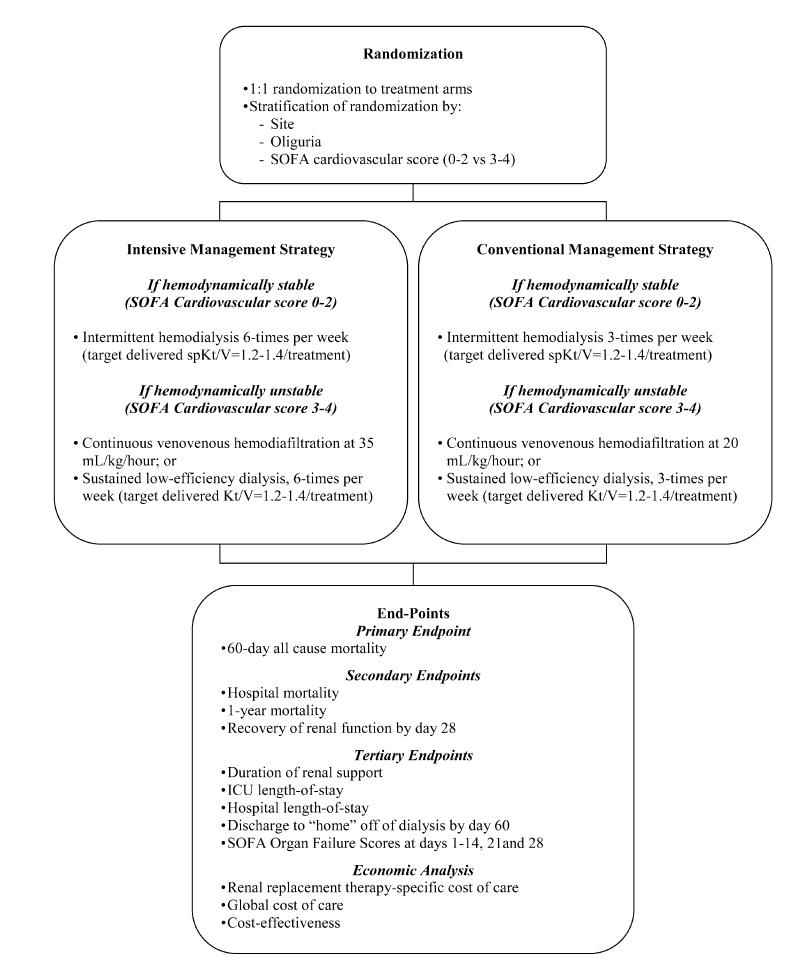
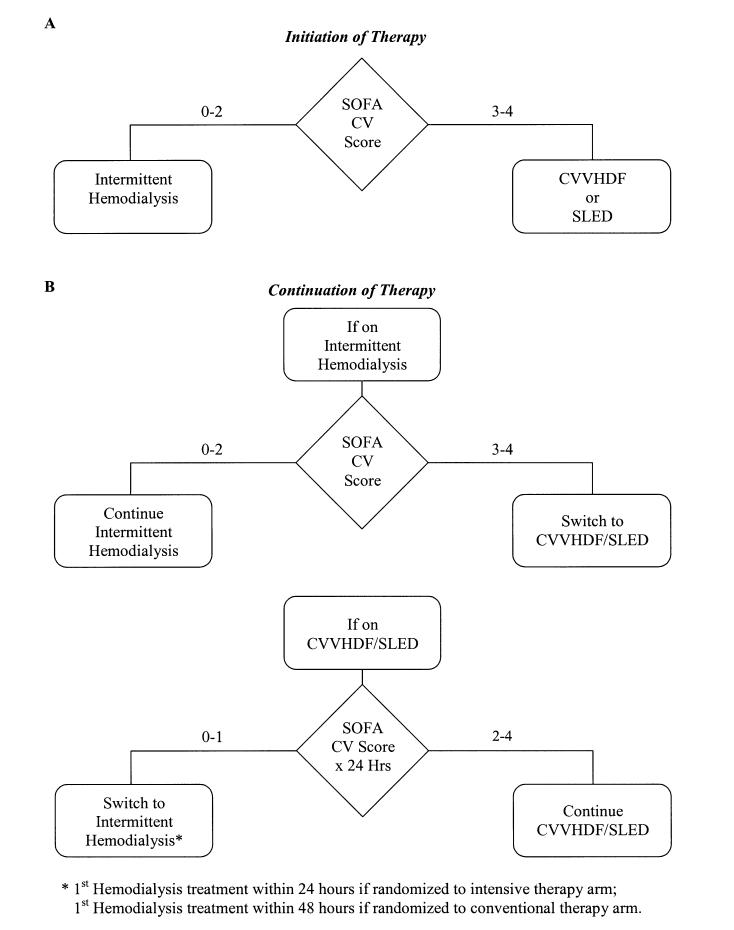
The optimal management of renal replacement therapy (RRT) in acute renal failure (ARF) is uncertain. The VA/NIH Acute Renal Failure Trail Network Study (ATN Study) tests the hypothesis that a strategy of intensive RRT will decrease 60-day all-cause mortality in critically ill patients with ARF. Dose separation between the two treatment arms is achieved by increasing the frequency of intermittent hemodialysis (IHD) and sustained low efficiency dialysis (SLED) treatments from three times per week to six times per week, and by increasing continuous venovenous hemodiafiltration (CVVHDF) effluent volume from 20 mL/kg/hr to 35 mL/kg/hr. In both treatment arms, subjects convert between IHD and CVVHDF or SLED as hemodynamic status changes over time. This strategy attempts to replicate the conversion between modalities of RRT that occurs in clinical practice. However, in order to implement this strategy, flexible criteria needed to be developed to provide a balance between the need for uniformity of treatment between groups and practitioner discretion regarding modality of RRT to maintain patient safety. In order to address safety and ethical issues similar to those raised by the Office of Human Research Protections in its review of the ARDS Network studies, a survey of practitioner practices was performed and observational data on the management of RRT in comparable critically ill patients with ARF managed outside of the research context is being collected prospectively. These data will help inform the study's DSMB and site IRB's of the relationship between the study's treatment arms and concurrent clinical practice.
Figures
References
-
- Star RA. Treatment of acute renal failure. Kidney Int. 1998;54:1817–31. - PubMed
-
- Lameire N, Vanholder R. Pathophysiologic features and prevention of human and experimental acute tubular necrosis. J Am Soc Nephrol. 2001;12(Suppl 17):S20–S32. - PubMed
-
- Karsou SA, Jaber BL, Pereira BJG. Impact of intermittent hemodialysis variables on clinical outcomes in acute renal failure. Am J Kidney Dis. 2000;35:980–991. - PubMed
-
- Mehta RL, Letteri JM. Current status of renal replacement therapy for acute renal failure. A survey of US nephrologists. Am J Nephrology. 1999;19:377–82. - PubMed
-
- Bonventre JV. Daily hemodialysis - will treatment each day improve the outcome in patients with acute renal failure. N Engl J Med. 2002;346:632–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
